Gun violence is up by 46% since 2004. As of late May 2023 , there have been 245 mass shootings. Gun liability insurance is a largely untried “middle path” approach that balances the right to bear arms with responsibility to mitigate risk. (Image: Brandon Bourdages/Shutterstock)
The blue columbines opened on my terrace. They’re among the first plants to flower each Spring, and their deep color and unique bird-like shapes are a cheery signal that winter has gone its way, and the season of renewal is upon us.
But this first flowering also strikes a discordant note because for me the word “columbine” inevitably evokes “Columbine High School,” and the horrific day in April 1999 when two Colorado teenagers walked into their school armed with 9mm semi-automatic weapons, and murdered 12 of their classmates and one of their teachers, for no apparent reason.
At the time, news of this massacre sent shockwaves through a bewildered nation: how was it possible that two kids could become so alienated, so angry that they would plan out and enact a wanton shooting spree and then kill themselves?
The media churned out speculations and analyses. Experts attempted to deduce motives. Political leaders wrung their hands and voiced condolences, along with impassioned affirmations that we as a nation “must do something” about gun control.
Mass shootings
no longer shock us the way they did in 1999. They’ve become too common.
In the 24 years
since Columbine, there have been 377 school shootings, according to the Washington Post. Over 349,000 kids nationwide have experienced
gun violence in the places they go to learn.
In 2023 alone, there have been 245 mass shootings, according to the Gun Violence Archive. That’s roughly 12 per week, on average, and the year’s not even half over. And these are the incidents that get reported.
And that’s in
addition to the hundreds more mass shootings—generally defined as incidents
involving guns that result in the deaths of four or more people, not including
the shooter(s)— in other public places like supermarkets, cinemas, nightclubs,
and banks.
In 2023 alone, there have been 245 mass shootings as of the Friday before Memorial Day weekend, according to the Gun Violence Archive—an independent non-profit that collects daily data from 7,500 law enforcement, government, and media sources. That’s roughly 12 per week, on average, and the year’s not even half over. And these are the incidents that get reported.
There have been 151 shooting incidents at schools in the US in the 24 years since the Columbine High School massacre in 1999 (Image TFoxFoto/Shutterstock)
Each mass
murder generates a surge of by-the-minute news flashes, then a predictable
canon of motive-mongering, displays of political piety, and detailed analyses
of how it all happened, who did what, and who’s to blame. Then comes the
redundant roar of arguments about gun control vs gun rights.
The headline-grabbing
massacres are on top of the staggering stats on gun-related incidents that
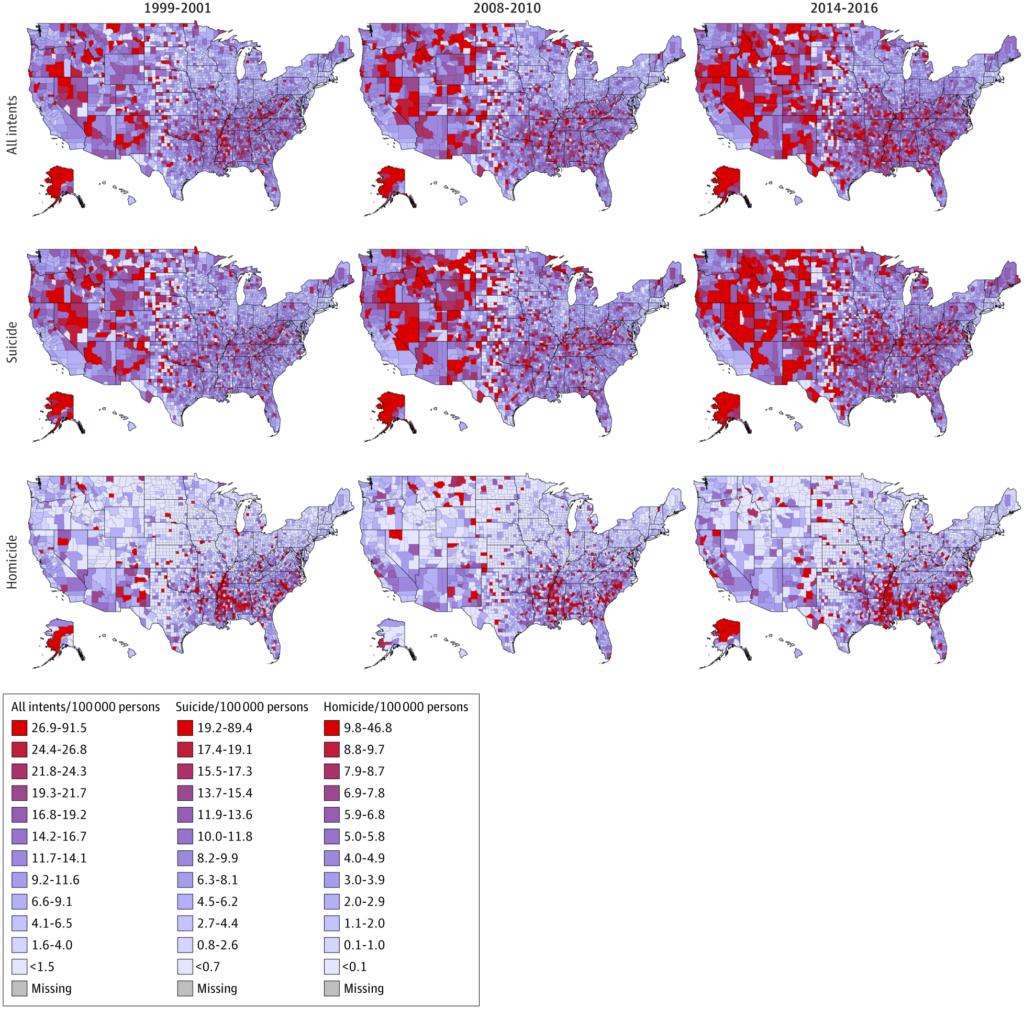
involve fewer than four victims. According to a comprehensive 30-year review published last November in JAMA Open,
there have been more than 1.1 million firearm-related fatalities in the US from
1990 to 2021. This includes intentional homicides, suicides, and unintentional
or accidental gun deaths.
Gun-related mortality
has increased by 46% since 2004, from a low of roughly 10 per 100,000 citizens
to a peak of nearly 15 per 100,000 in 2021 (Rees CA, et al. JAMA Open Netw.
2022).
Eric Fleegler,
MD, MPH, a professor of pediatrics and emergency
medicine at Harvard,
and one of the study’s authors told Holistic Primary Care that if other
any disease showed a steady mortality increase of the magnitude we’re seeing
with gun violence, it would spark a major public health response.
Gun-related mortality has increased by 46% since 2004, from a low of roughly 10 per 100,000 citizens to a peak of nearly 15 per 100,000 in 2021.
In fact, the gun violence issue has
elicited strong statements from several medical organizations. The American Public Health Association
has deemed it, “a major public health problem and a leading cause of premature
death.” In
its 2018 position paper,
the American Academy of Family Physicians states: “Gun violence is a national
public health epidemic that exacts a substantial toll on the US society.”
AAFP joined the American
Academy of Pediatrics, American College of Physicians, American College of
Obstetricians and Gynecologists, and the American Psychiatric Association in a
call-to-action, demanding that the president and congress:
Label violence caused by the use of guns as a national public health epidemic.
Fund appropriate research as part of the federal budget.
Establish constitutionally appropriate restrictions on the manufacturing and sale, for civilian use, of large-capacity magazines and firearms with features designed to increase their rapid and extended killing capacity.
Those are noble
intentions. But like many such statements in the past, they’ve done little to
stem the tide of gun-related bloodshed. As Rees, Fleegler, and colleagues show in
their study, gun violence has increased since the Covid pandemic all over the
country.
Last Spring,
President Biden signed into law the Bipartisan Safer Communities Act which increased funding for
community-based mental health services, and expanded background checks for gun
purchases by individuals under age 21, and bolstered states’ rights to impose
“red flag” rules preventing gun purchases by people with histories of violence
or severe mental illness.
The bill is
notable because it is the first significant piece of federal-level gun
legislation in 30 years, and because it was introduced in the Senate by Marco
Rubio (R-FL) and endorsed by 15 Republican senators.
In March of
this year, the Biden administration issued an executive
order calling for
near-universal background checks, wider use of “extreme protection orders,” tigher
regulation of gun industry marketing tactics, and strengthening of law
enforcement efforts to reduce the number of firearms “lost” or stolen during
shipping.
These efforts
are commendable. There’s no question that we need better mental health services,
and tighter control on who’s able to obtain guns.
It’s the Bullets
But these
measures—like much of the dialog about gun control—miss an important truth: it
is not the guns themselves that kill and maim, it’s the bullets. If we truly
want to do something about our heinous rates of violent deaths, we need to regulate
access to ammunition.
And there’s a
simple, market-based way to do that: Mandate gun-owner’s insurance in all 50
states, and require proof of insurance for ammunition purchases.
Now, if you’re a long-time HPC reader, you probably know
that I’m not a big fan of the insurance industry. In healthcare, insurance has
morphed into a ravenous profit-driven monster that all-too-often denies people
the care they need, while making physicians so miserable that one in
every five doctors is contemplating a career change.
But in the context of liability for gun violence, I
strongly believe an insurance-based approach, especially if coupled with
restrictions on ammo purchase, could potentially align financial pressures to
keep lethal hardware out of the hands of irresponsible, dangerous people.
A Middle Path
Gun rights advocates claim—and rightly so—that the
overwhelming majority of American gun owners are responsible people who keep
firearms to protect themselves and their families, or for hunting, or simply as
a hobby.
Gun liability insurance, coupled with requirements to prove that one’s guns are insured before buying ammunition is one very practical way for gun owners could prove they are, in fact, responsible. It would simultaneously provide a strong financial backstop to cover the medical and ancillary costs in case a 6-year-old kid happens to get hold of Daddy’s 9mm, takes it to school, and shoots his teacher.
It is not the guns themselves that kill and maim, it’s the bullets. If we truly want to do something about our heinous rates of violent deaths, we need to regulate access to ammunition.
What I’m suggesting here is a “middle path” approach, one
that balances the constitutional right to bear arms—a right that millions of
Americans hold sacrosanct—with the responsibility to ensure that those rights
do not infringe upon the safety and wellbeing of others.
An insurance requirement would not transgress the Second
Amendment. It would not involve “taking away” anybody’s guns. It would simply
introduce financial accountability into a milieu where, currently, there is very
little.
People would still be free to own as many guns as they
want, of whatever sort, so long as they are able to pay the insurance premiums.
And those premiums would be risk-assessed. A small handgun that a middle-aged
woman keeps for protection would not cost as much to insure as a military-grade
semi-automatic rifle newly purchased by a 19-year-old kid.
It could be just like automobile insurance—which sets a
strong precedent for harm-reduction and accountability via an insurance-based
system.
A Strong Precedent
Generally, most people accept the idea that insuring
one’s vehicle(s) is reasonable because cars and trucks can, and sometimes do,
cause harm to self or others. Likewise, most accept that car insurance premiums
vary depending on driver age and experience, type of vehicle being insured,
geographic location, past infractions, history of accidents, and other
variables. The same principles could be applied to guns—which unlike cars, have
no other intrinsic purpose than to injure and kill.
None but the most extreme libertarian considers car
insurance to be a Nanny State plot to squelch personal freedom.
This would also be a market-based, financially driven approach to reducing gun violence.
According to Statista’s 2022 data set, roughly 45% of American households own
guns, though the figure varies considerably by state. A recent article in The Guardian claims that Americans have bought more
than 150 million guns in the 10 years since the Sandy Hook shooting. According
to American Gun Facts, a Second Amendment advocacy group, there are roughly 446
million firearms in the US, and the average gun-owner possesses 5 weapons. AGF
notes over 21 million guns were purchased in 2020 alone.
That’s a LOT of
potential revenue for insurers. And we all know that the insurance industry
likes to make money.
Most people accept the idea that insuring one’s vehicle(s) is reasonable because cars and trucks can, and sometimes do, cause harm. Likewise, most accept that car insurance premiums vary depending on driver age and experience, type of vehicle being insured, and other variables. The same principles could be applied to guns—which unlike cars, have no other intrinsic purpose than to injure and kill.
Largely
Untested
But an
insurance-based system would require a top-down federal mandate. All 50 states
would need to enact and enforce it at the same time, or people in insured
states will simply go to uninsured states to purchase their hardware and
ammunition. Patchwork efforts would do very little.
Given the
current state of partisan politics in Washington, such a mandate—even if it
were proposed—is a distant dream.
At the same
time, some political observers say that Americans, regardless of party
affiliation, have seen enough carnage to finally bring the gun control issue to a new tipping
point.
(Image: Lightspring/Shutterstock)
Gun liability
insurance is not a new idea, but it is largely untested.
A 2013 New York Times article notes that at that time, several states
were toying with the idea of insurance requirements for gun ownership, though
none of these efforts came to fruition.
The move
represents the first such law in the nation, and while it’s an important symbolic
step, it is unlikely to have major impact. It a very local measure; it only
applies to liability from unintentional injuries; there’s no requirement for
proof of insurance to access ammunition; and its implementation has, not
surprisingly, met with opposition from gun rights groups (though a
federal judge recently upheld its constitutionality).
Gun liability insurance, coupled with requirements to prove that one’s guns are insured before buying ammunition is one very practical way for gun owners could prove they are, in fact, responsible.
Beyond the San
Jose experiment, a large-scale insurance-driven approach has never even been
tried. But Washington Post writers Jason Abaluck and Ian Ayres believe
that the concept could have greater public traction now.
In their
excellent 2022 article, The Case for Mandatory Gun-Liability
Insurance, they
state: Gun insurance would accomplish two goals: First, it would raise the cost
of gun ownership for people whose firearms are deemed relatively more likely to
be used in crimes (by themselves or others), based on an assessment of risk
factors made by insurance companies. That would make those people less likely
to obtain guns in the first place. Second, it would provide a strong financial
incentive for gun owners to keep these weapons out of the hands of people who
might commit crimes with them.”
Abaluck and
Ayers add that, compared with other regulatory measures such as all-out bans on
certain classes of weapons, an insurance-driven system “might win support from
conservatives looking for a market-based approach that wouldn’t have much
impact on responsible gun owners.”
“When you apply for homeowner’s insurance, they will ask whether you have a swimming pool, trampoline, or an aggressive breed dog. If you apply for life insurance, the agent is going to ask whether you smoke, are overweight or whether you’re a private pilot. They will ask if you scuba dive. But they won’t ask if you keep a firearm in your home or how it’s stored.”
““`Kristen Moore, University of Michigan
Again, the
car insurance analogy is helpful. Arguments against a reasonable gun insurance
mandate are easily flipped: “Oh, so you prefer irresponsible gun ownership and total
lack of accountability for possession of something that is designed to maim or
kill? Well, why should we bother to have car insurance? Why are businesses
required to have insurance against harm to customers or to the public?”
Viewed rationally, within the context of the broader
principles of liability insurance, the objections don’t really hold up.
Do the Numbers Add Up?
The bigger
question is whether insurance companies would see enough potential profit to
justify a long and ugly wallow into the quagmire of gun politics. Given the
sheer numbers of guns and gun owners, it seems like they’d have incentive. But
so far, insurers have stayed away from the gun issue.
Kristen Moore, PhD, Dept of Applied Mathematics, University of Michigan
Do a Google search for “gun insurance” and you’ll come up with lots of hits. But they’re for policies to insure the worth of gun collections in case they’re damaged or stolen. Policies that insure against liability for harm caused by guns are very, very hard to find.
University of Michigan mathematician Kristen Moore, PhD, who researches firearm trends, says that by and large insurers have taken a “don’t ask” stance toward guns.
“When you apply for homeowner’s
insurance, they will ask whether you have a swimming pool, trampoline, or an
aggressive breed dog. If you apply for life insurance, the agent is going to
ask whether you smoke, are overweight or whether you’re a private pilot. They
will ask if you scuba dive. But they won’t ask if you keep a firearm in your
home or how it’s stored,” she said in a 2018 interview.
Moore, an advocate for gun
liability insurance, goes on: “You pay a premium increase if you have a
trampoline and a premium increase if you have a swimming pool, but there are
measures you can take to ameliorate that risk. You can fence in your pool, for
example. Perhaps the same could be done for firearm ownership. If you take a
safety training class, or if you have a gun safe, then there might not be as
much of a premium increase.”
To the
extent that they’ve said anything about it, the insurance industry’s main
objection to gun liability insurance seems to be that insurers don’t want to be
on the hook for intentional acts of violence by gun owners. In other words,
they see gun ownership as high risk.
That alone speaks
volumes, and it’s all the more reason why we need some type of system of
enforced responsibility.
This would be a “middle path” approach, one that balances the constitutional right to bear arms—a right that millions of Americans hold sacrosanct—with the responsibility to ensure that the exercise of this right does not infringe upon the safety and wellbeing of others.
Moore
underscores the fact that gun violence already costs insurers. “People don’t
think about this, but the Columbine mass shooting resulted in a homeowner’s
liability claim. The Newtown mass shooting resulted in a homeowner’s liability
claim. Insurance executives have estimated that the Vegas shooting will result
in a billion dollars in claims across multiple lines of insurance.”
Perhaps
these occurrences are happening often enough that insurers might now see the
potential to make money from gun premiums as a way to offset the massive
payouts.
Aligning
Incentives
Over the
past year, I’ve talked to many people in diverse professions, and from various walks
of life about the general idea of gun owner’s insurance coupled with
requirements for proof of insurance before purchasing ammunition.
Most view the core principles as sound and sensible, though all agree that politically, any sort of gun control measure would meet with furious opposition from Second Amendment extremists, some of whom have gone so far as to call for abolition of the federal Bureau of Alcohol, Tobacco, and Firearms in its entirety.
To the extent that they’ve said anything about it, the insurance industry’s main objection to gun liability insurance seems to be that insurers don’t want to be on the hook for intentional acts of violence by gun owners. In other words, they see gun ownership as high risk. That alone speaks volumes.
Harvard’s
Dr. Fleegler says, gun liability insurance, “Makes enormous sense. If you get a
trampoline in your yard, or a pool, the insurance companies will raise your
rates. These things have injury rates much lower than guns.”
Eric Fleegler, MD, MPH, Assoc Prof of Pediatrics & Emergency Med, Boston Children’s Hospital
Even if
major insurers were to support a movement toward gun liability, implementation
of such a system would face logistical challenges beyond the inevitable
pushback from gun rights extremists.
As Abaluck
and Ayres point out in their Washington Post piece, such a system would
depend on insurers having access to gun trace data, and that would require
changes to the so-called Tiahrt amendments included in Department of Justice
appropriations bills since 2003. These amendments block anyone but law
enforcement agencies from receiving information obtained from gun traces done
by the Bureau of Alcohol, Tobacco, Firearms and Explosives.
It is true
that setting up an entirely new insurance-based system for responsible gun
ownership and ammunition access would face daunting difficulties. But we
desperately need a new approach to a social and medical problem that is raging
out of control. The alternative is more mayhem, followed by more ineffective
pontificating.
Gun
insurance won’t entirely solve the problem of gun violence. It won’t address
economic disparities, the epidemic of mental illness, or the nation’s cultural
obsession with violence as a preferred means of problem-solving.
There will
always be black market weapons, “ghost gun” assembly kits, and 3D-printed
weapons. And if gun insurance is mandated, there will inevitably be people who
shirk the laws just like there are people who now drive uninsured vehicles.
But a
comprehensive system of gun liability insurance could potentially drive greater
accountability and responsibility through financial incentives and penalties,
the one language that everyone seems to respect.
It’s a
middle-road, market-based, potentially bipartisan approach that does not
involve banning anything or infringing on constitutional rights. For reducing
the horrific burden of gun-related death and disability, it just might be our
country’s best shot.
A few weeks
ago, I was in a wine store. I went to the checkout counter with my selections,
and the cashier asked for my ID. I’m a few decades past age 21, as my grey
beard proudly announces wherever I go. So, I was quite surprised to be carded.
The cashier proceeded to scan my driver’s license, which struck me as very
strange.
When I asked
what was going on, she said she’s required to scan everyone’s ID—regardless of
age—in order to activate the cash register.
I walked out of
the store shaking my head, thinking “I wish they had a system like that to
control who can buy bullets.”
Doctor suicide is a
painful reality that hospitals, clinic networks, and medical schools go out of
their way to deny.
But with the emergence of a documentary called Do No Harm, and a surge of media attention following the suicide of Dr. Lorna Breen during New York City’s first COVID peak, healthcare leaders are finally being forced to reckon with the ugly truth that in many institutions, medicine has become a culture of abuse.
American physicians kill themselves at an alarmingly high rate. A least one doctor commits suicide every day in the US, according to research presented two years ago at the American Psychiatric Association’s annual meeting. Investigators at the Harlem Hospital Center in New York conducted a systematic literature review of physician suicides and identified a staggering rate of 28 to 40 per 100,000––more than twice the general population’s suicide rate of 12.3 per 100,000.
The review also showed that doctors have the highest suicide rate among all professions, including jobs in other high-stress fields like the military or law enforcement.
Those statistics were identified before COVID-19. In 2020, the pandemic is only accelerating existing trends. Stories of medical professionals lost to suicide in the last 5 months are shining new light on long-standing and dangerous shortcomings in our systems of medical education and practice.
Hazards of duty? Part of
the deal? Comes with the territory?
Only if that “territory”
is the United States.
Medicine is a high-pressure job anywhere. But doctors in other countries are not killing themselves at nearly the rates of their American counterparts. According to a 2019 systematic review by Dutheil and colleagues, US physicians are far more likely to commit suicide than their peers worldwide. Medical suicide rates have been rising in this country over the last decade; in Europe, they’ve actually been decreasing.
Why do so many American doctors
and medical students take their own lives? And why aren’t their deaths more
widely publicized?
Dr. Pamela Wible, a family physician by training, runs a helpline for physicians and med students contemplating suicide. Her recent book, Human Rights Violations in Medicine confronts the abusive medical culture that underlies physician suicidality
Wible believes guilt, bullying, and exhaustion are three leading causes of suicide in medicine. Physicians, med students, and other healthcare personnel are often subjected to abusive, even dangerous, working conditions. Overwork is common; self-care is penalized.
In many hospitals and
clinics, the inevitable pressures of medical practice are compounded by conflicting
administrative demands, hostile work environments, retaliatory office politics,
racial discrimination, and sexual harassment. It all adds up.
“‘Burnout’ is victim-blaming, and deflects attention from the hazardous working conditions that are illegal in any other industry that values safety, and the human rights violations that are rampant in medical education and beyond.”
—Pamela Wible, MD
Hazing & “Pimping”
It begins with the rigors
of medical education, and extends through insurance-based medicine’s emphasis
on volume over quality. Young physicians in training are frequently subjected
to sanctioned abuse and public humiliation in lecture halls and hospital wards.
They’re also severely sleep-deprived—itself a form of torture.
For some suicidal doctors,
the problems began when they entered medical school. Med students are typically
high-achievers accustomed to ranking at the top of their classes. Once in med
school though, some feel for the first time in their lives that they might not
really be smart enough, tough enough, or brave enough to become “good” doctors.
Within medical culture, there’s a pervasive fear of being weak, unintelligent, or incapable. That fear drives people to hide their mistakes and imperfections and shy away from seeking help, even when it’s desperately needed.
Some level of pressure and anxiety is to be expected in a career as demanding as medicine. But Dr. Wible sees shockingly toxic elements in US medical culture.
In her book Physician Suicide Letters, by Pamela Wible, MD responds to doctor suicide notes
Bullying, humiliation, and hazing are tolerated, sometimes even encouraged as acceptable training strategies. Many doctors can tell stories of getting “pimped,”––an aggressive, rapid-fire style of testing students’ clinical knowledge by asking difficult or intentionally unanswerable questions in class, in the clinic, and even in front of patients.
All that takes its toll.
A 2016 study of med students
by the National Institutes of Health and the US Department of State found that,
“overall prevalence of depression or depressive symptoms among medical students
was 27.2%, and the overall prevalence of suicidal ideation was 11.1%.” Among those
who screened positive for depression, only 16% sought treatment (Rotenstein, L et
al. JAMA. 2016; 316(21): 2214‐2236).
“There seems to be more
mental health distress among first and third-year med students, and definitely
for unmatched graduates. In some residency programs, 75% of residents meet
criteria for major depression,” Wible says.
Med students experiencing
depression, anxiety, or suicidal thoughts avoid seeking care because they worry
they’ll be “outed,” stigmatized, and punished if they do.
The stress and
pressure––and subsequent mental health risks––only increase once they
transition into actual clinical practice.
They enter an extremely hierarchical system in which they’re often forced to “earn their keep” by filling the most undesirable shifts. Long hours without breaks; weekend and holiday shifts with little time off; isolation from friends, family, and crucial social support—these are not exceptions, but rather the rule for many young doctors.
Sleep Starvation
Sleep deprivation is also a
big factor, says Wible.
It is not hard to find a
physician who can tell tales of falling
asleep, or witnessing colleagues
drop unconscious to the hospital floor, while making rounds, treating patients,
or conducting surgeries. Perhaps you’ve been one of them.
In other high-stress professions–pilots, air traffic controllers, even truck drivers, for example–there are regulations and work-hour restrictions that limit shift lengths, because everyone recognizes that sleep deprivation and overwork impair performance.
Yet our medical system
drives doctors—who routinely deal with matters of life and death that hinge on
clear, quick judgment—to the point of exhaustion.
Current ACGME requirements permit interns’ duty shifts to run for 24 consecutive hours––up from a previous cap of 16 hours––and 80 total hours per week.
Not only do we permit sleep-starved doctors to administer potentially dangerous drugs, monitor patients on a complex array of equipment, and perform surgeries that require great skill––we expect them to do it all flawlessly––and to be nice about it.
In other high-stress professions…there are regulations and work-hour restrictions, because everyone recognizes that sleep deprivation and overwork impair performance. Yet our medical system drives doctors—who routinely deal with matters of life and death that hinge on clear, quick judgment—to the point of exhaustion.
Exhausted doctors are more
likely than well-rested ones to make medical errors, which sometimes kill patients.
A 2018 Mayo Clinic study found that physicians who made errors were more likely
to exhibit symptoms of fatigue, burnout, and recent suicidal ideation (Tawfik, D et al. Mayo
Clin Proc. 2018; 93(11): 1571-1580).
When Epidemics Collide
COVID-19 presented new and unusual stressors for clinicians in viral epicenters like New York City, Washington, DC, and Chicago, where prevalence was highest during the early months of the pandemic.
Emergency medicine
physicians and nurses are particularly vulnerable. In centers with very high caseloads
they’re working under constant duress, sometimes without adequate protective
equipment, in hospitals that were understaffed even before the pandemic. As
they treat their patients, they worry about their own risk, and the potential
for carrying the virus home to their families.
Dr. Wible, who has
provided counselling for suicidal clinicians for nearly a decade, says that since
the coronavirus, she’s seen a dramatic increase in the number of calls.
“Volume doubled, and I led
group support calls on Zoom to handle the uptick in requests for support,” she
reported.
On April 26, Dr. Lorna Breen, a well-respected ER doctor at New York Presbyterian’s Allen Hospital in New York City died of “self-inflicted injuries” at age 49. Her story got the media’s attention, as it represented the convergence of two epidemics: COVID and doctor suicide.
Lorna Breen, MD, an ER physician who committed suicide at the height of New York’s COVID spike, was an accomplished orchestral cellist
Prior to her death, Dr.
Breen had treated many coronavirus patients, and she herself had recently
recovered from the virus.
“Make sure she’s praised
as a hero, because she was,” Breen’s father, also a doctor, told the New York Times. “She’s a casualty just
as much as anyone else who has died.” The elder Dr. Breen also stressed that
his daughter, “did not have a history of mental illness.”
In its official public statement,
New York Presbyterian used similarly valiant language. “Dr. Breen is a hero who
brought the highest ideals of medicine to the challenging front lines of the
emergency department.”
But an email to hospital staffers did not immediately identify the cause of Breen’s death, reflecting an attitude of denial and obfuscation that Wible says is the rule, not the exception, among hospital administrators.
Breen’s family and
hospital “had to use ‘healthcare hero’ propaganda on her immediately, so that
she wasn’t forgotten or thrown to the wind as weak,” Wible told Holistic
Primary Care.
“They gave her the hero spin because she was in New York City and had a high position in her hospital. Her family made it clear that she never had any preexisting medical conditions and instead suggested her death was due to the coronavirus, to distance her and the family from the topic of mental health issues.”
This denial contradicts
evidence Wible has gathered from the nearly 1,500 cases she has recorded. She finds
that ER doctors rank among the top three medical specialists most likely to die
by suicide. Psychiatrists, surgeons, and anesthesiologists also have a higher
risk than others.
Secondary Trauma
Wible believes secondary
trauma plays a big role, at least for the latter two specialties.
Breen’s family insists
that she never suffered from prior mental health challenges, but Wible says it’s
hard to imagine that a doctor who spent her entire career in the ER never
suffered a single blow to her emotional or cognitive wellbeing.
“I believe all emergency
medicine doctors have mental health wounds,” Wible said.
It is common to hear
clinicians say that experiencing or witnessing a catastrophic injury or illness
early in life is what inspired them to pursue medical careers. Wible finds that
“many EM doctors have experienced significant trauma in their childhoods––then
they go into emergency medicine and are re-traumatized every day.”
Even those who did not
experience childhood trauma will invariably incur “occupationally-induced
mental health wounds” while working in the emergency department. “If they have
not sought appropriate care, then they are still wandering around with those
wounds every day,” she said.
It’s Not “Burnout,” It’s Abuse
“This is tough work, even
on the best day,” Wible says of the medical life. “Even in the parts of
medicine that seem like they could be happy, there is unforeseen, extreme
tragedy.”
In our current systems,
the inevitable stresses and pressures of caring for sick, injured, and
sometimes dying people, are amplified by factors unrelated to patient care.
Micromanagement by senior
doctors or hospital administrators; incessant demands for documentation; veiled
threat of punishment or legal consequences for errors; poorly managed and
understaffed clinics; incessant time pressures. All these factors leave many
physicians feeling not only emotionally exhausted, but cynical towards the
profession they once loved.
We call it “burnout.” But Dr.
Wible warns that this term obscures the abusive nature of our medical system
itself.
“‘Burnout’ is victim-blaming,
and deflects attention from the hazardous working conditions that are illegal
in any other industry that values safety, and the human rights violations that
are rampant in medical education and beyond.”
Hospitals treat physicians
in ways that “break the UN Declaration
of Human Rights,” she suggested. Other medical professionals also experience extreme
pressure, overwork, and abuse. But statistically, the suicide risk is much
higher for physicians.
Hidden in Plain Sight
Part of the problem is
physicians’ uncanny ability to hide their suffering not only from colleagues
and supervisors, but from family members and friends. Doctors who experience depression,
anxiety, or suicidal ideations often view those symptoms as flaws that must never
be exposed. Some worry that admitting psychological or emotional distress will call
into question their fitness to practice or, worse, might lead to dismissal.
The faces of some of the young physicians and medical students who have committed suicide in recent years. Comnposite image from the film, Do No Harm, by Robyn Symon
There may also be
expectations from family and friends that someone who has “made it” in such a
high-status profession must surely be reaping rewards. Some doctors feel a sense
of duty not to disappoint parents, spouses, or other loved ones who’ve also invested
and sacrificed to make their medical careers possible.
As a result, few people know
when a doctor friend or family-member is contemplating suicide.
Dr. Wible—who had her own struggles with anxiety and suicidality earlier in her career—says there are a few red flags: “Excessively happy doctors are often hiding their emotions and pain.” Additional warning signs may include a recent medical liability case, medical board complaints or investigations, and major life events like divorce.
Denial: A Double Assault
Denial by hospital
administrators, family members, and colleagues has only compounded the problem
of doctor suicide.
“We create the scenario
that takes these wonderful young people and puts them in a situation where they
can see the only way out is death––and then we bury their suicides,” Wible
said. “It’s like a double assault.”
She pointed out that a
number of doctor suicides involving ingestion of prescription drugs were misleadingly
reported as “accidental” overdoses. It is certainly possible for physicians to
unintentionally take too much medication, but this explanation stretches credibility.
MDs get extensive training in pharmaceutical use; that makes them some of the
least likely people on the planet to unknowingly over-consume a drug.
Doctors do, however, have
ready access to controlled substances, which heightens risk of abuse. According
to a 2013 study published in the Journal of Addiction Medicine, 69% of
doctors reported that they abused prescription drugs “to relieve stress and
physical or emotional pain” (Merlo, L et a. J Addict Med. 2013; 7(5): 349-53).
Physicians also possess an
intimate and detailed knowledge of human anatomy, increasing the chances that
they will complete a suicide if attempted.
Concealing doctor suicides
protects medical schools and hospitals from having to address systemic problems.
But sweeping the dirty secrets under the rug only puts other health
professionals––and their patients––at tremendous risk.
“Suicide is not the
problem; censorship is,” Wible argued. “If we would just speak openly about
this crisis, it could be easily solved.”
Effective, evidence-based
suicide prevention tools exist––and they can help avert the needless loss of
doctors’ lives. “We have the resources to solve this problem. But if we censor
it, we can’t make it better. We can’t solve a problem that nobody is acknowledging.”
Get Up, Stand Up
Wible says that to truly
shift medical culture in a healthier direction, “we need to normalize the
conversation about suicide risk, just like we’ve normalized conversations about
blood pressure.”
Doctors, medical students, and family members gather for a candlelight vigil commemorating clinicians lost to suicide, in a scene from the film, Do No Harm
Education is also vital.
Two resources she recommends are the documentary “Do No Harm” by filmmaker, Robyn Symon, and her free audiobook of doctor suicide
notes, Physician Suicide
Letters—Answered, in which she shares her correspondence with numerous clinicians whom
she’s helped to avoid suicide.
The key, she says, is providing
a forum for self-expression without fear of rebuke or humiliation. “The system
of medical education and practice should be set up in a way where people are
able to connect with each other honestly, emotionally and spiritually, without
punishment,” Wible said.
Fixing the situation will
also require system-wide reforms to create more humane working conditions
within medical institutions. Wible believes doctors, nurses, med students,
and other health professionals need to stand up and fight for those reforms.
The book documents a spectrum
of abusive situations–from food and sleep deprivation to threatening
foreign-born doctors and trainees with deportation–that routinely occur in
American clinics. It also gives guidelines to help doctors chronicle their own
experiences of abuse, and practical action steps for confronting and resolving
these situations.
Dr. Wible is certainly not
the only physician concerned with doctor suicide, and pushing for change.
Keith Frederick, an
osteopath who also served for eight years in Missouri’s House of
Representatives, introduced a bill to address mental health in Missouri medical
schools after learning that a fourth-year osteopathic student in his community
died by suicide just days before graduation.
In the film Do No Harm,
Dr. Frederick described suicide as an unacknowledged “occupational hazard” in
medical settings. During his years as a legislator (2011-2019), he also
sponsored a bill requiring hospitals to examine mental illness and burnout
among staff.
Not surprisingly,
Frederick’s proposal met initial resistance from Missouri medical institutions.
The deans of all six of the state’s med schools co-authored a letter urging
legislators not to pass the bill.
Kevin Dietl (2nd from left), with his family. In April 2015, the 26 year old 4th year osteopathic studen took his own life. His parents, John & Michelle, have become leaders in the effort to reform medical education and practice, and to destigmatize mental illness within the culture of medicine.
Ultimately, though, Frederick
and his supporters won-out. The “Show-Me Compassionate Medical Education
Act” (MO Senate Bill 52) was signed into law in
July 2017. It requires medical schools to provide incoming students with
information about available depression and suicide prevention resources. It
also granted medical institutions the authority to conduct internal research,
without penalty, on rates of depression, suicide, and other mental health
issues among medical students.
Thank a Doctor, Save a Life
In addition to raising
awareness around suicide risk and prevention, expressions of gratitude can literally help keep
doctors alive.
Wible encourages people to
“please show appreciation and give thank you cards to your doctors, and ask
them how they are doing.”
It might seem simplistic
or even silly, but she believes it can be life-saving.
“It can be very hard to reach doctors––they’re often so closed off emotionally. It’s important that they feel validated, normal, and appreciated.” A thank you letter may give a doctor a much-needed dose of positive reinforcement that he or she may not otherwise receive.
Verbal thanks are nice
too, but Wible says that penned messages carry an even greater and
longer-lasting power. “Thank you notes are huge––especially if they are
written. They have a lifespan that goes on for decades––doctors will read and
reread them, sit and stare and really soak in the words.”
Clinics and hospitals
might also consider setting up anonymous compliment boxes where staff and
patients alike can submit thank you notes to their doctors or colleagues.
She also urges medical
practitioners to prioritize their own health and self-care. She herself does
this by “spend[ing] a lot of time in nature, hiking, gardening, and with my
animals.” She also stressed the importance of strong social connections, like
the one she shares with her loving partner.
“And most
important,” she added, “I get therapy WEEKLY.”
She holds that all med
students and doctors should receive “non-punitive, 100% confidential
therapy” every week. Whether it’s for preventive or active treatment,
breaking down the barriers around mental health support could help avert the
tragic doctor suicides on which our current systems prefer to turn a blind eye.
Bone and joint health are often reduced to simplistic
suggestions, like “take calcium,” “eat more dairy,” or “take something to build
collagen.”
But there is so much more to it. Bone is a living,
metabolically active tissue in a reciprocal relationship with the joints, and
connective tissues.
In this FREE webinar, David Craig, NMD, will share a growth
factor paradigm for restoring bone and joint health based on the use of Bone
Morphogenic Proteins (BMPs).
Drawing from his decades of clinical experience as a
naturopathic physician, as well as his own personal quest to better understand
the key factors influencing health and disease, Dr. Craig will explain how BMPs
can address the root causes of poor bone/joint health.
During this webinar, you’ll learn about:
The root causes of bone health – beyond minerals
The key determinant of joint health – beyond supplementation
The growth-factor connection – essential stem-cell signals
A growth-factor paradigm for regenerative medicine utilizing Bone Morphogenic Proteins (BMPs)
SPONSORED BY Regenerative Tissue Sciences, the professional sales division of ZyCal Bioceuticals Healthcare Co., Inc
David Craig, NMD earned his doctorate in naturopathic medicine at the University of Bridgeport College of Naturopathic Medicine. This 8-year training program included the internships and ER rotations in conventional allopathic clinics, and classes taught by professors from Yale Medical School, along with intensive education on natural therapies. He has been in private practice for 22 years, specializing in endocrinology, immunology, chronic fatigue syndrome, nutrition counseling, and the identification and mitigation of environmental triggers that can cause the body to become unhealthy.
Stanford researchers have found evidence that an RNA sequence called “Xist,” which is only produced by biologically female (XX) mammals, is an important factor in the etiology of many autoimmune diseases (Image: Sergii Laramenko/Shutterstock)
The
statistics have been clear and consistent for decades: autoimmune conditions are
at least three times more common among women than men. Some studies suggest
it’s more like a factor of four. For specific diseases like Lupus, the
disparity is 9-fold. For Sjogren’s syndrome, it’s 19 to 1.
This
appears to be an objective biological phenomenon. It’s not a reflection of
gender-based differences in seeking medical care, or of misdiagnosis—though
there’s plenty of that. Neither is it strictly hormone-related.
Hormonal
factors do play some role in autoimmune disorders. But the hormonal differences
between biologically female and male individuals in no way fully account for
the marked disparity of autoimmune diseases.
In
humans, and in rodent models, the simple presence of the double X chromosome is
far more predictive of autoimmune risk than any measure of hormone status.
A
Vexing Question
What
accounts for such a marked gender disparity? It’s a question that has vexed
researchers, clinicians, and patients for a long time.
An
international research team headed by two dermatologists at Stanford University
believe they have an answer, or at least a strong clue.
They
contend that Xist—a specific form of long non-coding RNA produced by
biologically female mammals—is the decisive factor.
Xist
has a very particular function: it squelches gene expression on one of the two
X chromosomes in each cell, thereby preventing a lethal doubling of proteins
coded by genes within the X chromosome. This X chromosome inactivation occurs
during early embryogenesis.
Through
a process that appears to be random, each cell in the embryonic female body
“decides” which of its two X chromosomes it will inactivate. The one selected
for silencing begins to produce Xist, which then binds to and coats the
chromosome, thus inhibiting transcription of its genes.
This
“decision” is preserved over the lifetime of the individual, through many
cycles of cell division, ensuring that all of the cells in the body are only
transcribing one set of X chromosome genes into actual proteins.
X
Inactivation & Autoimmunity
In
humans, Xist is a 19 kb long non-coding (lnc) RNA chain. The length of the
chain differs slightly in other mammals, but the function is the same.
Biologically male animals have the gene for Xist on their X chromosomes, but
under normal circumstances it is never expressed. Production of Xist only
occurs when two X chromosomes are a matched pair inside a cell.
So,
what does this have to do with autoimmune disease?
Once
Xist binds to the X chromosome that will be silenced, a wide range of other
types of proteins bind onto Xist, forming ribonucleoprotein (RNP) complexes. It
turns out that many of these are autoantigenic.
Dr.
Dou is a researcher in the lab of Stanford dermatologist and geneticist, Howard Y. Chang, MD, PhD.
Nearly a decade ago, Chang, Dou, and their colleagues identified nearly 100
proteins that can bind to and accumulate around Xist. A more detailed bibliomic
analysis showed that 30 of these Xist RNPs had been previously identified as
targets for autoantibodies associated with human autoimmune diseases including Rheumatoid Arthritis, Systemic Lupus Erythematosus, Multiple
Sclerosis, Myositis, and Sjogren’s syndrome.
This was not entirely surprising. The authors note that
autoantibodies are often directed toward nuclear RNA binding proteins. “The
nature and titer of such autoantibodies define the type and severity of
autoimmune diseases in clinical practice.”
But the fact that these particular autoantibodies
targeted a specific type of RNA complex that binds to the X chromosome, and is
normally produced only by biologically female mammals, opened an entirely new
line of inquiry about the etiology of autoimmune disease.
“Human
patients with autoimmune diseases displayed significant autoantibodies to
multiple components of XIST RNP. Thus, a sex-specific lncRNA scaffolds
ubiquitous RNP components to drive sex-biased immunity,” they wrote.
This
hypothesis was bolstered by the fact that in men with Klinefelter syndrome—a
rare genetic condition defined by having one Y and two X chromosomes—the risk
of many autoimmune disorders is comparable to that of women. Men with
Klinefelter’s are phenotypically male. Though their testosterone levels are
usually low, they do show typically male hormone patterns. It seems that in
this population, the predisposition to autoimmunity is connected to the
presence of that second X chromosome.
Dr.
Chang, who is a clinician as well as a researcher, said his driving interest in
this question is a desire to help his patients. “As a practicing physician, I
see a lot of lupus and scleroderma patients, because those autoimmune disorders
manifest in skin,” he said in a
Stanford University press release following publication of the new study
last February. “The great majority of these patients are women.”
Xist
Increases Autoimmunity
To
prove that Xist can generate autoimmune responses, the Stanford team assembled
an interdisciplinary, international consortium of researchers who, together, undertook
some very sophisticated bioengineering.
First,
they developed transgenic strains of mice in which the males produced Xist in a
similar manner as the females. The particular Xist gene which they inserted
into the mouse genome is inducible by external chemical means. In this case,
the chemical trigger was doxycycline, which the investigators could give to the
mice in drinking water. This gave the them the possibility of turning on or shutting
off Xist production in the males. Once induced, Xist forms similar RNP
complexes in the males as seen in female mice.
The
investigators then injected the test mice with pristane, an irritant that can
induce a lupus-like autoimmune reaction in susceptible mice. In this way they
could test whether male mice that produced Xist were more likely than normal
males to show the autoimmune response.
Indeed,
they were. The male mice with activated Xist were far more likely to show autoimmune
reactions following pristane stimulation than the non-Xist males. The
autoimmune reactions occurred at a rate comparable to that of females similarly
stimulated with pristane.
“Increased
disease severity and elevated autoreactive lymphocyte pathway signatures were
observed in the mouse models of pristane-induced SLE,” the authors report. “Expression
of Xist RNPs in male mice is sufficient to increase disease severity and change
the expression and epigenomic profiles of both the B cell and T cell
effectors of SLE pathogenesis.”
Chang
and colleagues note that the presence of Xist alone does not induce
autoimmunity; the Lupus-like syndrome still needed to be stimulated by the pristane
injection. But the presence of activated Xist in genetically male mice that
would not ordinarily express Xist did increase the likelihood and severity of
the autoimmune reaction once the pristane stimulus was applied.
The
findings give creedence to the core hypothesis that production of Xist, and the
subsequent RNP complexes it forms, predisposes an organism to autoimmune
reactions.
New Human
Disease Markers
On its
own, this mouse experiment could be dismissed as a very elaborate science fair
project with limited clinical significance. But the Stanford team went a step further:
based on the antigens they identified in the mice, they designed an antigen
array to test serum obtained from humans with autoimmune diseases, which
allowed them to assess reactivity to specific Xist RNP complexes.
Using
this array, they were able to compare serum from patients with Dermatomyositis,
Scleroderma, or SLE, with samples obtained from healthy donors who did not have
autoimmune diagnoses.
They
found that the autoimmune patients were significantly more reactive to 79 of
the antigens tested than the healthy control subjects. Of those 79 antigens, 53
were associated with Xist RNPs. Nine of the protein complexes tested were antigenic
in all three of the disease categories. Further 28 of the 53 Xist-associated antigens
had not previously been described in association with specific autoimmune
diseases.
“These
results show that multiple proteins from the Xist RNPs are novel autoantigens
in patients with DM, SSc, and SLE.” This suggests that some of them could eventually
become potentially new markers for detecting autoimmune conditions.
The
Stanford research goes a long way in making the case that Xist and its related
protein complexes, play a role in the etiology of autoimmune disorders, though it’ll
take more work to definitively prove it.
Nature
vs Nurture?
The
findings are provocative in that they suggest that the strong gender disparity
in incidence of autoimmune disorders could be gene-linked, and therefore
independent of diet, lifestyle, or environmental factors.
In an interview shortly
after publication of the study, Dr. Chang stated: “This research says that the
risk for autoimmune disease comes from your genes. It’s not something you did
wrong. Sometimes people are like, “Did I eat something wrong? Did I do
something wrong?” No. It’s not something you can control.”
That
runs somewhat counter to core principles of functional, holistic, and
naturopathic medicine which put autoimmunity in the context of modifiable
factors like microbiome dysregulation, intestinal impermeability, food
allergies, and exposure to things like mold and environmental toxins.
Understandably,
the paper generated considerable interest within the functional medicine
community.
Terry Wahls, MD, a professor of medicine at
the University of Iowa, who reversed her own Multiple Sclerosis via nutritional
and lifestyle changes, and has taught MS patients to do the same, described the
Stanford study as “Super interesting.”
Though
the clinical implications are not entirely clear, Wahls says the paper underscores
the broad problem of “not having enough women in studies.
A blind spot was created,” she told Holistic Primary Care.
Joel
Evans, MD, a functional medicine practitioner specializing in women’s
health, says the Xist research prompted a lot of conversation among his peers
and colleagues. Though it clearly suggests that predisposition to autoimmunity
is X-linked, this is definitely not a clear-cut nature versus nurture dyad. The
predisposition may indeed be genetic, but exogenous factors still play a big
role in determining whether or not someone will actually manifest an autoimmune
disease, Dr. Evans says.
Indeed, while autoimmune conditions are more common in
women than men, the majority of women do not have autoimmune diseases despite
having an XX genotype and producing Xist RNA. Further, some men do have
autoimmune conditions, though they do not produce Xist. In fact, one autoimmune
disease—Type 1 diabetes—has a higher incidence in males versus females.
Studies of identical twins show that the development of
autoimmune disorders is not always identical in twin pairs, despite the shared
genome.
The discovery that Xist-linked protein complexes can function
as autoantigens is compelling. It adds a new and very interesting piece to the
autoimmune puzzle. But it is not the entire picture.
The presence of microplastics in carotid atheromas is comparable to diabetes in terms of raising the risk for stroke and myocardial infarction, according to a new study published in the New England Journal of Medicine. (Image: Ukrolenochka/Shutterstock)
The
presence of micro- or nano-plastic particles in carotid atheromas significantly
raises the risk of myocardial infarction, stroke, or death from any cause
within 3 years.
That’s
the blunt conclusion of a new multi-center study headed by researchers at the
Department of Advanced Medical & Surgical Science, University of Campania,
Naples, and involving more than 250 at-risk patients undergoing carotid
endarterectomy.
Micro-
and nanoplastics (MNPs), defined as plastic particles smaller than 5 mm and
1,000 nm respectively, result from the mechanical breakdown of larger plastic objects.
MNPs are increasingly found in air, water, soil, and food worldwide.
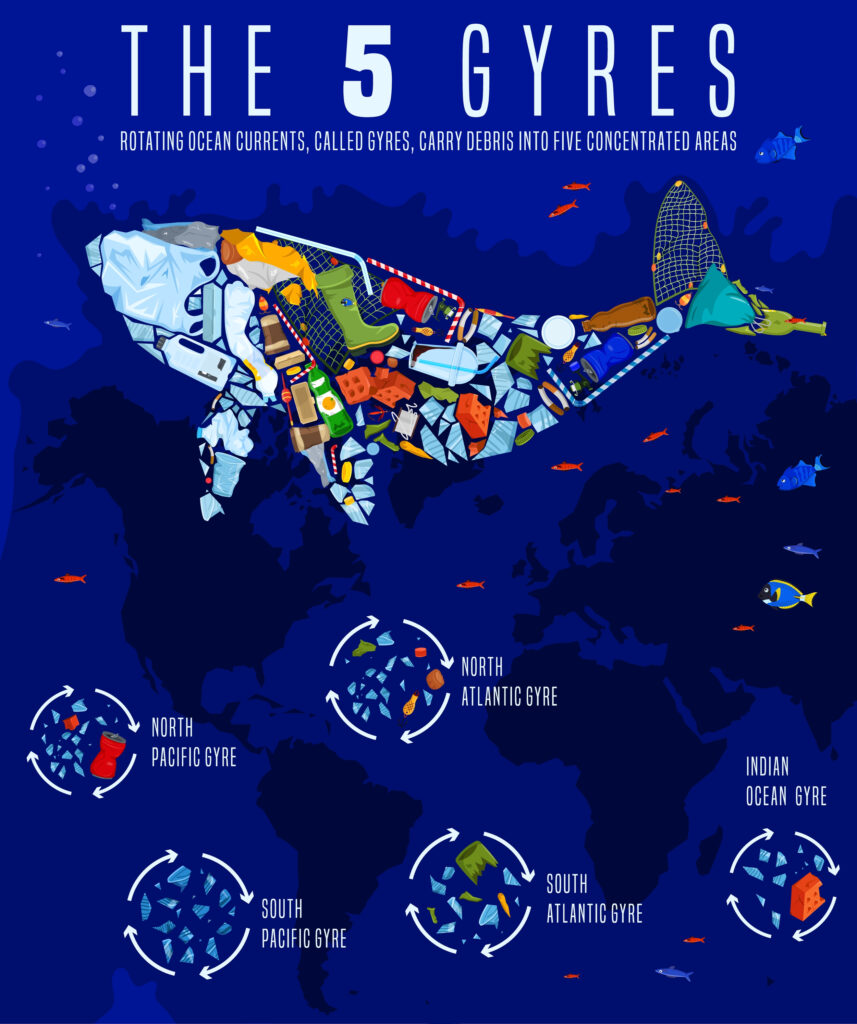
According to a
2014 estimate,
there are between 15 and 51 trillion individual bits of microplastic in the
world’s oceans. They’re estimated to weigh between 93,000 and 236,000 metric
tons. That was 10 years ago, and that’s not accounting for the much smaller
nanoplastics. The problem has only increased since then.
Chronic
exposure to MNPs via ingestion, inhalation, or skin contact, is also
increasingly common. Over the last decade, researchers around the globe have
detected MNPs in human lung,
liver, and placental tissue, as well
as in blood,
urine, breast milk, and feces. They’ve
also been found in tissue of wild birds, fish, and mammals.
Animal
studies and in vitro models suggest that specific MNPs may be
cardiotoxic, primarily because they can trigger oxidation, inflammation, and
apoptosis in endothelial cells, and can also induce myocardial fibrosis. Constant
MNP exposure has been linked to a number of respiratory, digestive, and
immunologic disorders.
Plastic
in Plaques
The
new study, published in the March 7 edition of the New England
Journal of Medicine, is the first
human clinical study to provide firm evidence that MNPs are an independent
factor for adverse cardiovascular outcomes in at-risk people.
Rafaelle Marchella, MD, PhD
The multicenter
team, headed by veteran cardiovascular researcher, Raffaele Marfella, MD, PhD,
analyzed atheromatous plaque tissue for the presence of MNPs, using several
methods: pyrolysis, gas chromatography, mass spectrometry, stable isotope
analysis, and electron microscopy. They looked for 11 specific types of micro-
or nanoplastics. Two types—polyethylene and polyvinyl chloride—showed up at
high levels in a large number of the patients.
Marfella’s
team initially enrolled 312 patients from three different hospitals, all of
whom underwent endarterectomies to mitigate the risk associated with advanced
though asymptomatic carotid atherosclerosis and stenosis (greater than 70%).
Eight of these patients died prior to discharge, and 47 were either lost to
follow-up or not available for complete data collection.
The
researchers followed the remaining 257 people for a total of 34 months. They
tracked incidence of nonfatal stroke, nonfatal myocardial
infarction, and death from any cause, distilling these into a composite
endpoint.
Well
over half of the patients (58.4%) had atheromas containing polyethylene, at a mean
level of 21.7 ±24.5 μg per milligram of plaque. Thirty-one (12.1%) also had
detectable levels of polyvinyl chloride, at a mean level of 5.2 ±2.4 μg per
milligram of plaque.
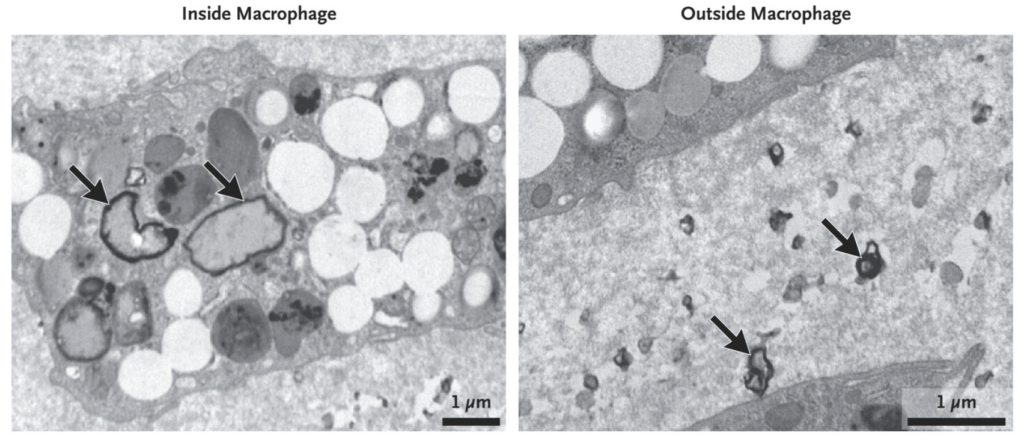
The
authors note that the minute plastic particles were, in fact, visible to
microscopists. “Electron microscopy revealed visible, jagged-edged
foreign particles among plaque macrophages and scattered in the external
debris.”
Transmission electron micrographs showing microplastic particles (arrows) inside and outside of living macrophages with atheromatous plaque tissue obtained from a patient who had undergone carotid endarterectomy (From, Marfella R, et al. NEJM. 2024)
The people who carried MNPs were more likely to be male,
more likely to smoke, and more likely to be diabetic and severely dyslipidemic
than those who did not. But there were no differences between the two groups in
terms of body mass index or severity of carotid stenosis. In both groups,
the mean age was in the early 70s (71 years old for those with NMPs, 73 for
those without).
There were no geographic
differences in the prevalence of MNPs based on the locations of the three
clinics at which the patients were treated.
A Health Hazard
Beyond
the astonishing fact that people these days are exposed to so much plastic that
it ends up in their carotid arteries, we must consider the possibility that the
presence of microplastics is very detrimental to human health.
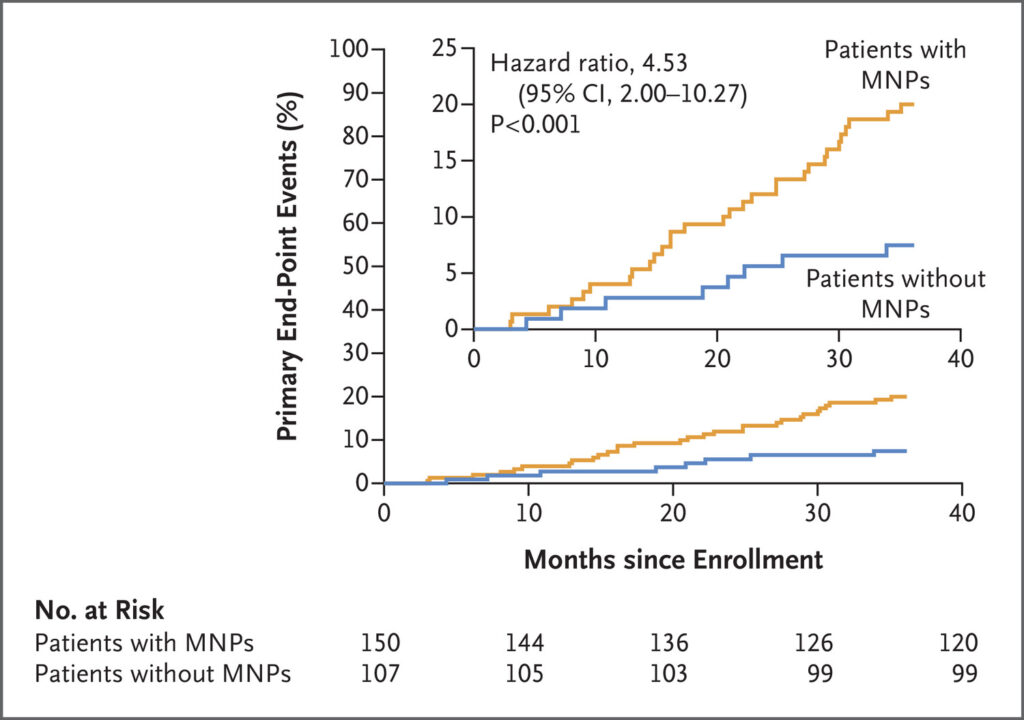
Marfella’s data show that compared with
subjects who were MNP-free, those who had plastic in their plaques had a
4.5-fold increased risk for the composite adverse endpoint (hazard ratio, 4.53; 95% confidence interval, 2.00 to
10.27; P<0.001).
The authors stressed that outcomes were logged via reviews of electronic medical records by reviewers who
were unaware of the MNP status of the patients in question.
Among the 150 subjects showing MNPs, there were 14
non-fatal strokes, 10 non-fatal MIs, and 6 deaths. Among the 107 people without
MNPs, there were only 5 strokes, 2 MIs, and 1 death.
The incidence of stroke, MI, or death from any cause
was 20% among the patients with MNPs, versus 7.5% in those without the plastic
residues in their arteries. That’s close to a 3-fold difference.
Put another way, the authors calculated there were 6.1
events per 100 patient-years in the MNP subgroup, versus 2.2 events per 100
patient-years in the MNP-free cohort.
Comparable to Diabetes
How predictive is the presence of MNPs for
morbidity and mortality? Very predictive, it seems.
Marfella and
colleagues stress that their data do not prove that MNPs cause stroke or
MI. But their Cox regression analysis showed that the presence of MNPs confers
a hazard ratio for adverse outcomes comparable to that of diabetes (4.53 and
4.76, respectively). MNPs were more predictive of adverse outcomes than age,
BMI, total cholesterol, and several other common cardiovascular risk
factors.
The Italian
researchers also provide further evidence that MNPs are proinflammatory. They
measured serum IL-8, IL-1β, IL-6, and TNF-α in blood samples from the study’s participants. They also measured
collagen content in the atheromatous plaques, and levels of CD3 and CD68, all
of which are indicators of inflammation.
All cytokines increased
in correlation with the amount of polyethylene present in the plaque samples,
as did the CD3 and CD68 levels. The collagen level went down as MNP levels
increased. All of these findings support the notion that MNPs drive
proinflammatory pathways in human tissue.
Several
previous epidemiological
studies concluded that occupational exposure to plastic-related pollutants
including polyvinyl chloride can raise the risk of cardiovascular disease. The
Marfella provides clinical evidence to bolster that hypothesis.
Direct &
Indirect Effects
MNPs may have direct
and indirect effects on cardiometabolic health: they can clearly translocate
directly into the circulation and into the endothelial tissue, and they may
also trigger systemic inflammation which is a key factor in the development and
progression of heart disease.
The degree to
which MNPs can infiltrate human tissue is largely dependent on particle size:
the smaller the particles, the more deeply they are able to penetrate into our
organs.
Marfella and
colleagues state that the nanoplastic particles they observed in the
atherosclerotic plaques from their patients were well below the 200-nm
threshold for passage through the gut barrier layer and into the bloodstream.
Ubiquitous
& Insidious
This study adds
to the groundswell of research in recent years, showing that plastics in our
environment—and remember, there are no endogenously produced plastics—are absorbed
by our bodies, and that they can affect our physiology.
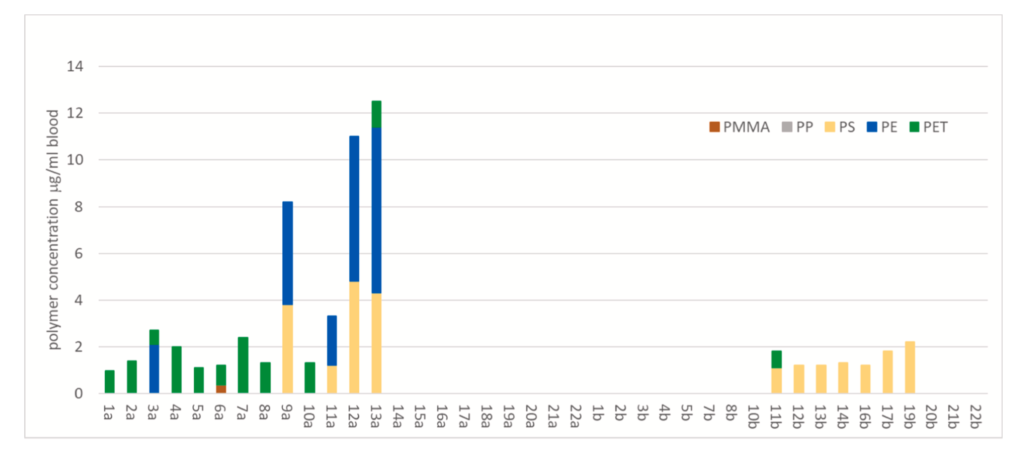
Heather Leslie
and colleagues had analyzed blood samples from 22 healthy adults, and found
plastic residues in 17 of them (77%). Half contained traces of polyethylene
terephthalate (PET), a common material for food containers and beverage
bottles, and one quarter showed microparticles of polyethylene.
Concentrations of plastic particles by polymer type in whole blood samples of 22 donors. PMMA=poly methyl methacrylate; PP =Polypropylene; PS=Polystyrene; PE=Polyethylene; PET= polyethylene terephthalate (from Leslie H, et al. Environ International. 2022)
The Leslie
study built on earlier evidence, including a 2009 paper documenting plastic
additives, especially phthalates, in the urine of 242 pregnant women (Meeker
JD, et al. Philos
Trans R Soc Lond B Biol Sci. 2009), and a 2019 study showing an
average of 20 different microplastics in feces from eight healthy human
volunteers (Schwabl
P, et al. Ann Intern Med. 2019).
There are many
different types of micro- and nanoplastic. Why were polyvinyl chloride and
polyethylene the only ones that Marfella and his team detected in carotid
atheromas?
It’s a good
question with no definitive answer….yet.
“Studies in
animal models suggest that the physicochemical features of different MNPs
influence whether they reach distant organs,” say the authors. “Additional work
is needed to assess whether polyethylene and polyvinyl chloride accumulate
preferentially within plaque and whether they are more pathogenic than other
types of MNPs in this regard.”
Another big
yet-to-be answered question is whether MNPs are themselves directly
atherogenic, or simply absorbed into existing atherogenic plaques without
playing any direct role in stimulating plaque formation.
The presence of
MNPs in circulation and in atherosclerotic plaques may also be an indicator of
other environmental, dietary, and lifestyle-based risk factors. In other words,
it may be a reflection of a generally unhealthy lifestyle.
“The
association between the presence of MNPs within plaque and the incidence of a
composite of cardiovascular disease or death outcomes may also entail the risk
from exposure to other residual, unmeasured confounding variables, such as
unknown exposures during the life course of the patient or, more broadly, the
health status and behaviors of the patients,” Marfella and colleagues write. They
add that this study did not look specifically at diet or lifestyle-related
variables.
Modes of
Exposure
Polyethylene
and polyvinyl chloride, the two types of MNPs that the Italian researchers
detected in carotid atheromas, are ubiquitous in modern industrial societies.
They’re used to make food and cosmetic containers, water pipes, and a host of common
household and industrial items.
MNPs resulting
from the breakdown of polyvinyl chlorhide and polyethylene have been identified
in drinking water, in foods, and cosmetic products all over the world. Particles
of 2.5 μm or less can also be aerosolized, meaning that they can be inhaled,
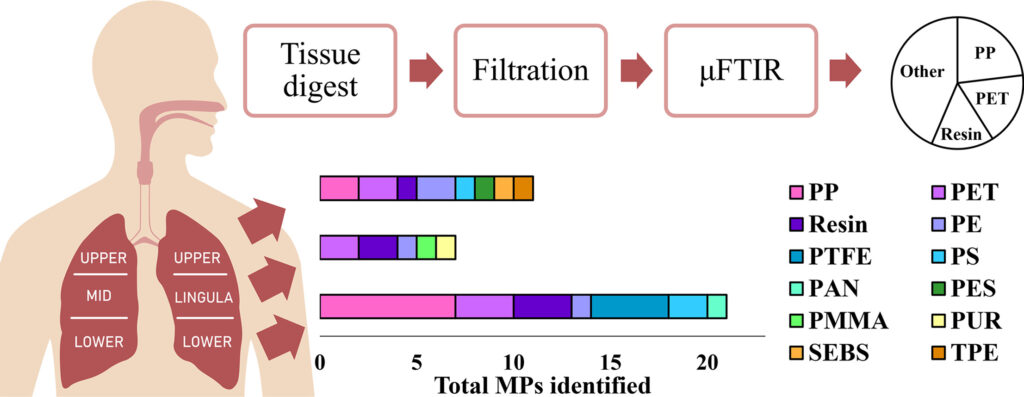
entering the lungs and the blood. Lauren Jenner and colleagues at the Hull York
Medical School in the UK, identified polyethylene microparticles, along with polypropylene
in lung tissue samples from 13 people (Jenner
L, et al. Sci Tot Environ. 2022).
(From Jenner L, et al. Sci Tot Environ. 2022)
Like many other environmental toxins, microplastics and
nanoplastics have the potential to bioaccumulate up the various food chains,
with concentrations being highest in apex species, like humans. Some studies have
suggested that on their way up the food chain, MNPs absorb and accumulate other
toxic substances including persistent organic pollutants (POPs) such as
polychlorinated biphenyls (PCBs) and pesticides. In other words, they become
carriers for other potentially problematic substances. (Lithner
D, et al. Sci Tot Environ. 2011; Koelmans AA, et al. Environ
Sci Tech. 2013).
Though
researchers are just beginning to understand the full impact of microplastics
on human health, there’s already reason for concern. Some types of microplastic
can disrupt and destabilize
the lipid bilayers comprising cell membranes. Others increase oxidative
stress, trigger apoptosis, and alter immune system function (Danopoulos
E, et al. J Hazardous Materials, 2022).
Possible Microbiome
Effects
Plastic
breakdown products might also be harmful to our gut microbial ecology, says
Vanessa Stadlbauer-Köllner, MD, a clinical gastroenterologist in the Department
of Gastroenterology & Hepatology at the Medical University of Graz,
Austria.
“From animal
studies it’s already known that microplastic causes changes in the gut
microbiome. When you feed mice with microplastic they develop microbiome
changes. And when you look at this microbiome it looks like that of somebody
who is obese or has cancer, or has some other diseases like diabetes. You see a
loss in diversity, an increase of potentially pathogenic species,” Dr. Stadlbauer-Köllner told Holistic Primary
Care.
“Could it be
that microplastic in our environment is one of the factors that causes obesity
and metabolic disorders?”
Public Health
Implications
Given the ubitquity of
plastics in our surroundings, exposure to MNPs begins practically at birth, and
it increases as we age.
Dr. Marfella and his
colleagues speculate that this could be one of the many factors that underlying
the very well-established correlation between age, carotid stenosis, and cardiovascular
disease in general.
Ocean currents have concentrated plastic waste, along with other garbage, into five massive oceanic gyres (Image: Double Brain/Shutterstock)
They also point out that some
people are much more likely to be breathing and ingesting MNPs than others.
Certainly, anyone who works in manufacturing of plastics, or at other jobs that
involve constant engagement with plastics will be at greater risk of MNP
exposure.
Generally speaking, Blacks,
Asians, Hispanics, Latinos, and low-income populations are exposed to higher
levels of fine particulate air pollution than Whites and economically well-off people.
The Italian researchers hold
that while there are not yet any epidemiological studies looking specifically
at racial, ethnic, geographic or socioeconomic differences in MNP exposure, it
is reasonable to extrapolate from patterns observed with other pollutants, that
the aforementioned groups experience greater MNP exposure as well.
The biggest question prompted
by the Marfella MNP study is, what to do about it? This question applies at both the personal and
public health levels. Plastics are everywhere in our environments. Production
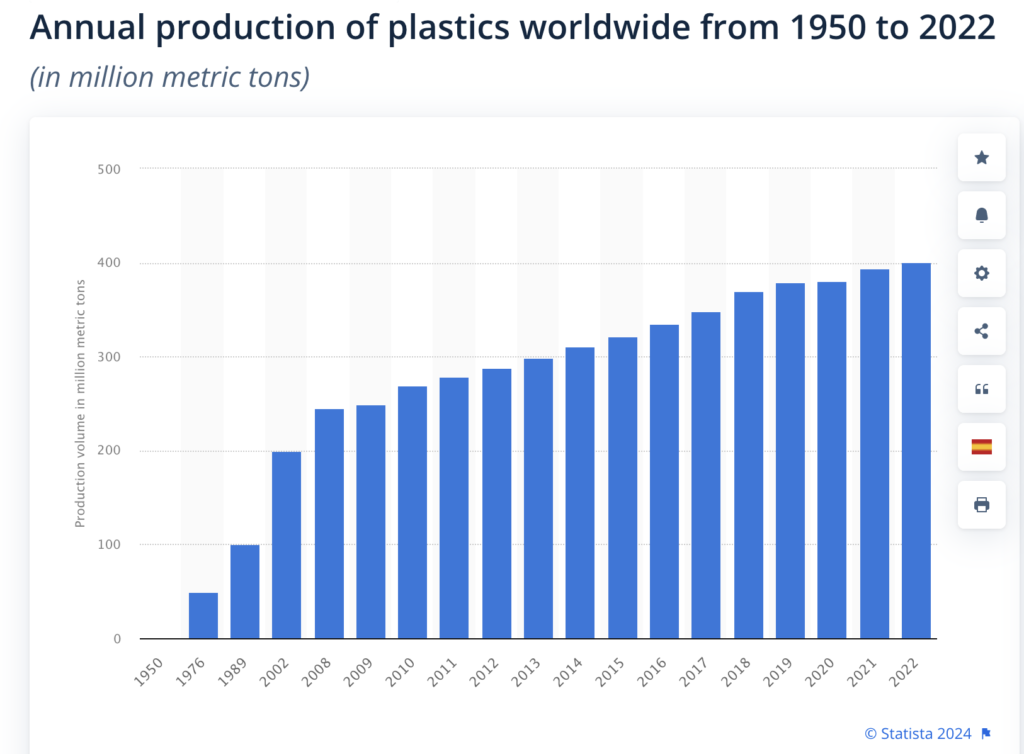
and use of plastics has not declined over the years. In fact, it has increased
steadily since the 1950s. Global
production of plastics doubled in the 20 year period from 2002 to 2022,
from 200 million metric tons to 400 million metric tons.
China is now the biggest
plastic producer, accounting for 32% of all plastic materials in 2022; the US
contributes roughly 17%.
If MNPs are indeed an independent
risk factor for cardiovascular disease, it is one that our species will be
contending with for a long, long time.
Microbes to the
Rescue?
A glimmer of
hope in this otherwise dismal picture is coming from some very cutting edge
microbiome research showing that certain bacteria, including a particular
strain of Pseudomonas
aeruginosa, are able to form
biofilm “nets” that can trap and bind microplastics.
Building on
work by Professors Song Lin Chua and James Kar-Hei Fang at the Hong Kong
Polytechnic Institute, Dr. Stadlbauer-Köllner and her colleagues at the Medical
University of Graz, are planning studies to look at bacterial strains that
could potentially digest microplastics.
“There are some
enzymes present in some bacteria that can digest certain kinds of plastics. And
some of these bacteria belong to families that occur in the human gut
microbiome,” she told Holistic Primary Care. “So, we will screen common gut
commensals to see whether they have the genes to produce the enzymes that
digest plastic. Then we will feed them with plastic and see if they can really
degrade it.”
Though this is
obviously a long way off from clinical application, it could very well turn out
that it’ll be the microbes that spare us from our own environmental and physiological
folly.
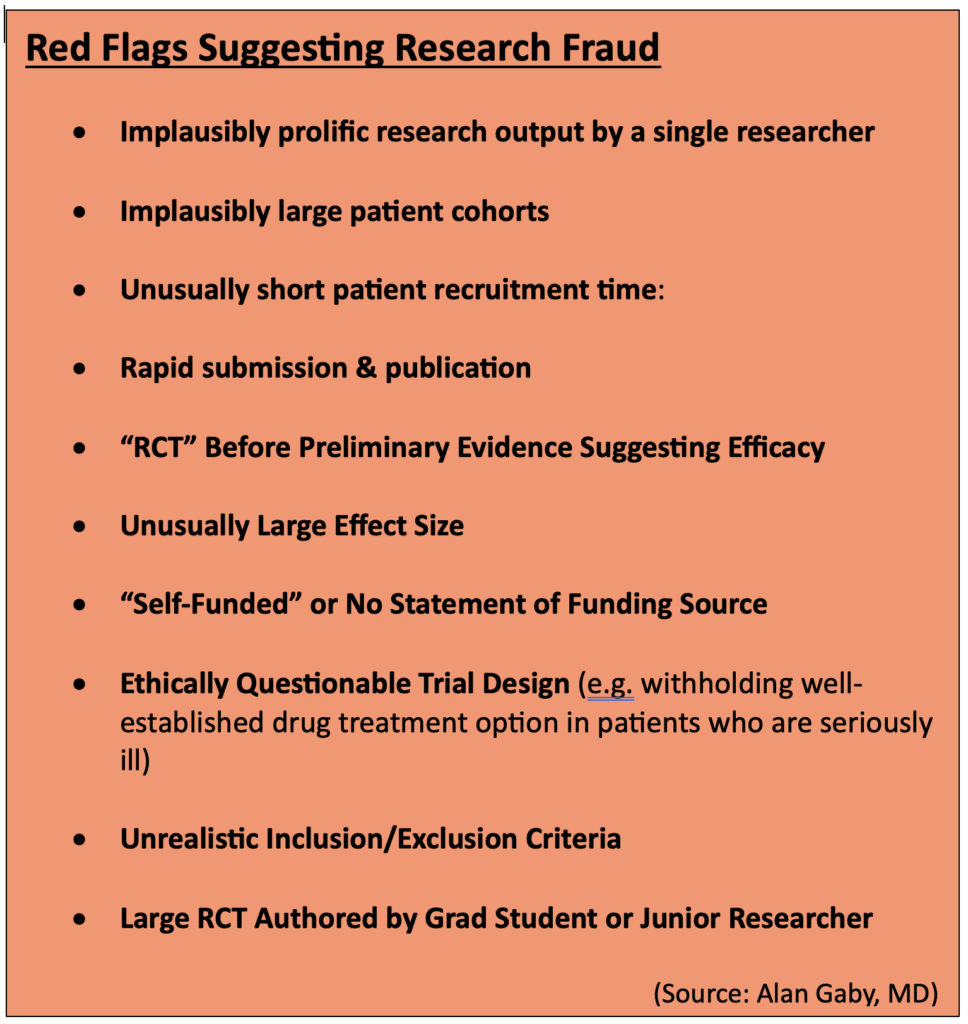
The proliferation of fraudulent clinical research has reached epidemic proportions, creating a major headache for practitioners. There were roughly 10,000 fraudulent papers retracted by medical journals last year, the highest number on record. While the problem affects all areas of medicine, the field of nutrition is especially vulnerable (Image: PeopleImages–Yuri A/Shutterstock)
Good
medical practice is based on trust.
Patients trust that practitioners are knowledgeable, and that they put their knowledge in service of their patients’ best interests. In turn, practitioners trust that clinical researchers run their studies honestly, and that the editors and peer-reviewers of the medical journals carefully scrutinize the papers they receive, sift out the garbage, and only publish studies that pass clinical, statistical, and ethical muster.
Research is, in itself, a trust proposition. From the lead investigators who design trials, and the Institutional Review Boards (IRBs) that approve them, to the research assistants and post-doctoral fellows who crunch the data, and the authors who write and submit the papers for publication, there’s a thread of trust that depends on the right people doing the right things at each point along the path.
That’s
how it ought to be in an ideal world. But the hard truth is, this is not an
ideal world.
It’s
an open secret that medical research fraud is rampant.
A recent article
in The Guardian estimated that last year, there were more than 10,000 fraudulent
papers retracted by journals across the sciences. That’s the highest number of
retractions ever recorded. And this is likely just the surface layer of the
problem.
Epidemic
Proportions
Alan Gaby, MD, author of the textbook, Nutritional Medicine. Dr. Gaby has read and reviewed tens of thousands of nutrition papers over the years. “Several hundred papers per year….raise questions about whether the research is legitimate.”
Research
fraud is widespread across many domains of healthcare, but it is especially
problematic in the field of nutrition, says Alan Gaby, MD, a holistic physician who is author of the massive textbook, Nutritional Medicine.
Now
in its third edition, Gaby’s book contains nearly 17,000 research citations and
covering the use of herbs and nutraceuticals for more than 400 specific health
conditions. Suffice to say, Dr. Gaby has probably read more clinical research
papers on nutrition than anyone on the planet.
He
contends that the problem of research fraud has reached epidemic proportions.
“Over
the past 50 years, I’ve probably reviewed about 50,000 papers. And about 15
years ago, I became aware of some irregularities in a lot of the research. A
growing number of papers left me wondering if the research had actually been
done at all, or if the data were simply fabricated.”
Fraudulent research corrodes public trust; it misleads clinicians; and it skews metanalyses. Once marketers and sales people get hold of it, they easily turn it into dishonest and misleading product claims. At minimum, ordinary people get ripped off. At the extreme, people could get hurt.
Gaby
says the number of suspicious—or at least highly questionable–papers has
surged dramatically in recent years, in part due to the growth of open access publishing and the proliferation of small, poorly refereed open-access
journals and websites, some of which are pay-for-play operations.
But
open-access is only part of the problem. Gaby says he’s seen numerous instances
in which dubious nutrition studies have appeared in venerable, “high impact”
(ie, widely-cited) conventional medical journals.
“Several
hundred papers per year, in my view, raise questions about whether the research
is legitimate.”
Gaby
stressed that it is difficult—and time consuming—to prove definitively that a published
paper is fraudulent. But there are an alarming number of studies that simply do
not hold up to careful scrutiny. When this happens in respected peer-reviewed
journals, as it sometimes does, it suggests that peer reviewers are failing to
do their jobs, or that they’re turning a blind eye to shoddy work.
Dr.
Gaby is not the only physician ringing alarm bells. Several years ago, a team
of researchers based in New Zealand called out two prominent Japanese
investigators—Yoshihiro Sato and Jun Iwamoto—claiming that nearly 300 of their
published papers in 78 medical journals, had major methodological flaws, ethical
lapses, and signs of fabrication.
Sato,
who died in 2017, and Iwamoto were both prominent professors at Japanese
universities. Their work was primarily focused on bone metabolism, and they
published many studies looking at the effects of Vitamin D, Vitamin K, and folate.
They also studied prescription drugs like methylprednisolone, hormone
replacement therapy, and valproic acid. Some of their research extended into
fields like neurology and gastroenterology.
Alison Avenell, PhD, University of Aberdeen, Scotland. Dr. Avenell headed an effort to expose one of the biggest legacies of research fraud in history
Studies
by Sato and Iwamoto have appeared in some of the world’s top journals,
including the Journal of theAmerican Medical Association (JAMA),Neurology, and the Journal of Bone and Mineral Metabolism.
The
saga began in 2006, when biochemist Alison Avenell, the Chair of Health Services Research at the University of
Aberdeen, Scotland, was delving into the question of whether vitamin D could
reduce bone fractures. While plumbing the literature, she came across two
studies by Sato. One involved a cohort of stroke patients, and the other, patients
with Parkinson’s.
Avenell
noticed that in both studies, the patient populations had exactly the
same mean body mass indexes. That, she thought, was statistically unlikely. She
started digging more deeply, and the more she looked, the more anomalies she
found: unreasonably large treatment effects, unusually large patient
populations, plagiarized text, numbers that simply didn’t add up.
“Expressions
of Concern”
Soon
after, Avenell teamed up with Andrew Grey, Mark Bolland, and Greg Gamble of the
University of Auckland, New Zealand. The team undertook an exhaustive review of
292 papers published by Sato alone or in partnership with Iwamoto.
In
2016, this intrepid team published an in-depth takedown of 33 studies by Sato,
Iwamoto, or both. They notified 78 journals that most, if not all, of the
nearly 300 papers published by these two researchers were flawed at best,
fraudulent at worst.
Not
long before he died, Yoshihiro Sato admitted that he falsified research, and
absolved Jun Iwamoto of any direct responsibility.
German anesthesiologist, Joachim Boldt, MD, formerly at the Klinikum Ludwigshaven, holds the global record for most papers retracted. A shocking 194 of Boldt’s published studies have been deemed fraudulent.
The
so-called “Sato Affair” is one of the biggest legacies of medical research
fraud in history. According to Retraction
Watch, a
website founded by former Medscape VP, Ivan Oransky and science writer Adam
Marcus, that monitors retractions across a vast range of scientific
disciplines, Sato and Iwamoto hold the 4th and 6th places
for highest number of papers retracted worldwide.
Who’s number one? That dubious honor belongs to Joachim Boldt, a German anesthesiologist and ICU physician, who’s had a stunning 194 of his published papers retracted because of data fabrication and lack of ethics board approval.
Red
Flags for Fraud Detection
With
fraudulent research on the rise across the medical landscape, and peer review
boards apparently faltering, practitioners need to sharpen their critical
thinking skills when reading clinical studies. But one need not become a
statistician.
“Several hundred papers per year, in my view, raise questions about whether the research is legitimate.”
–Alan Gaby, MD
Over
the years, Dr. Gaby has identified ten red-flag warning signs that raise the index
of suspicion about misconduct or outright fraud:
Implausibly prolific research output by a
single researcher: A good clinical researcher typically completes and publishes 3-4 large,
randomized, double-blind, controlled trials in a period of 5 or 10 years, Gaby
says. Yet, some researchers publish 10, 20, or even 30 papers in that time
span. “Whenever you see implausibly large research output, it makes you wonder
how could they have possibly done all of that research.”
Implausibly large patient cohorts: Gaby says
that over time, people who read a lot of studies develop a good sense of how
many people could be reasonably enrolled in a given trial. This is based in
part on the number of researchers and clinics involved, the size of those
clinics, their catchment areas, the general prevalence of the disease in
question, and the stringency of inclusion/exclusion criteria. In some nutrition
studies, a lone researcher claims to have a trial population far larger than one
could reasonably expect even in a multi-center study, let alone a trial at a
single clinic.
Unusually short recruitment time: Recruiting
patients for legitimate clinical studies is not easy, nor is it swift. It takes
a lot of outreach, effort, and resources. If a study claims to have recruited hundreds
of people with a particular disorder in a 3-month period, and they all met strict
inclusion criteria, you should be suspicious.
Rapid submission & publication: Most studies disclose
the time period for patient recruitment, and the duration of treatment lasted.
From that, you can estimate the earliest possible date of completion. Gaby says
he sometimes sees studies in the nutritional literature that were submitted for
publication very soon after it would be possible to complete the trial, based
on the schedule described in the text.
“In some cases, we’ve seen papers that were submitted before
it was possible to have completed the trial. In many other cases, only a few
weeks to a month after the trial could have been completed. That’s also
implausible, because in a real study, it takes a very long time to analyze
data, to write the paper, and then to submit it.”
An RCT before there is preliminary evidence of
efficacy: Real
clinical trials are costly. Few funding sources are likely to underwrite that
cost without some compelling preliminary evidence from case reports, open-label
uncontrolled trials, or pilot studies showing that the intervention in question
might be beneficial. Yet, in the nutrition and botanical literature, there are
many alleged RCTs done without such preliminary evidence.
Effect sizes larger than one would expect from nutrients: “If you read
a lot of medical literature, you start to get a general idea of how effective
nutrients are. Sometimes it’s dramatic, but most of the time it’s not. Usually,
it’s a combination of nutrients producing a moderate effect,” says Gaby. Yet,
“in many of the studies I’ve looked at, there were much larger effects…effect
sizes you usually only get from drugs. So that raises eyebrows.”
No funding source is listed, or the study is “self-funded”: This is
particularly important when researchers describe their studies as RCTs. Real RCTs
are very expensive. If nobody is funding it, one has to wonder how the study
was possible. And if funding sources are not openly stated, one needs to wonder
why.
The trial design raises ethical issues: If a study involves
patients with serious, advanced disease, and they’re randomized to either a
nutrient or a placebo, there’s likely an ethical problem. That’s because clinical
research is still in the domain of patient care, and doctors have a
responsibility to treat people with the best available therapies. Whether
natural medicine advocates like it or not, the “best available” treatments for
serious diseases are usually prescription drugs. If researchers intentionally
withhold a viable drug option in order to test a nutrient against a placebo,
they’re treading on shaky ethical ground.
Implausible patient characteristics: Pay close
attention to the stated inclusion and exclusion criteria, especially the age
range and baseline characteristics. Dr. Gaby says he sometimes sees papers that
indicate a particular age range for inclusion, but the when he looks at the
mean ages and the standard deviations in the results, it would be
mathematically impossible that all participants actually met the stated age
criteria.
A large study—especially an RCT—authored by a
grad student. Grad
students are the unsung heroes of clinical research. While they certainly
deserve credit for their efforts, the reality of academic hierarchies is that
they are seldom lead investigators, especially on big trials. Yet in the
nutrition literature, one will often see big studies authored by a grad student
or junior researcher, sometimes as the sole investigator. While this is not a
universally damning indicator, it should raise the index of suspicion a bit,
especially if there are other red flags.
Countries
of Origin
Dr.
Gaby says there’s another important indicator of potential scientific fraud:
geography.
“The
most common country of origin, by far, for questionable papers, is Iran. To a
lesser extent, Egypt and China. Then India, Pakistan, Japan, and Italy.”
Though
a German holds first place for total retractions, and other Japanese
researchers aside from Sato and Iwamoto also rank high on Retraction Watch,
Iran is now the world’s leader in terms of the sheer volume of questionable
papers flooding the literature, says Gaby.
“It’s
gotten to the point that if something comes out of Iran, I’m inclined to not
bother even reading it. Which is too bad, because probably some of the studies
are legitimate. But my estimate is that at least three-quarters and probably
more of the studies coming out from Iran these days, and to a lesser extent
from Egypt, Japan, Italy, and others, raise serious concerns about whether the
studies were actually done.”
Iran
has an advanced healthcare
system—a
mix of public, private, and non-governmental non-profit payers. On some public
health metrics, it ranks higher than the US. Roughly 90% of all Iranian citizens
there have some form of healthcare insurance.
Unfortunately,
the country also has a highly competitive market for well-paying, high-prestige
jobs that require advanced degrees and scientific prominence. That, along with
a totally unregulated cottage industry of for-hire study writers, is a major
driver of fraudulent research from Iran.
“The most common country of origin, by far, for questionable papers, is Iran. To a lesser extent, Egypt and China. Then India, Pakistan, Japan, and Italy.”
–Alan Gaby, MD
The
problem is not new. In 2016, Richard Stone the International News Editor for Science
magazine authored an article called, “In Iran, a
Shady Market for Papers Flourishes.” In it, he reveals a lucrative business centered on fabricating
research and getting it placed in the international literature.
For
the equivalent of around $600 (1.8M Iranian Tomans), scientific aspirants can
commission a paper or thesis that ‘doesn’t need lab work.” An additional $400 increases
the odds that the paper will be published “under your own name” in a
“reputable” journal. That means, a journal published by an internationally
recognized publisher like Springer or Elsevier.
“Paper
Mills”
Stone
says there are several thousand of these ‘paper mills’ throughout Iran, mostly
centered around prominent academic institutions. He cites a prominent member of
Iran’s Academy of Sciences who, in 2014, estimated that roughly 10% of all
masters and PhD theses awarded in the country –amounting to about 5,000 theses
per year—are based on research that the candidates never did.
This
is completely legal. There are no laws in Iran—or other countries for that
matter–against fabricating scientific data or publishing bogus research. Stone
notes that in 2016, a group of Iranian scientists concerned about scientific
integrity proposed a law to criminalize—at least partially—the selling of
concocted science. It never saw the light of day.
In
his review in Integrative Medicine, and in his lectures, Dr. Gaby draws
attention to several Iranian researchers who published prolifically on
nutritional topics, and whose work is very likely fraudulent.
Asemi’s
Astonishing Output
Among
them, Zatollah Asemi, a metabolic
disease specialist at the Kashan University, who published more than 191 “RCTs”
over his career, including 148 studies published between Jan 2016 and March
2019.
Zatollah Asemi, MD, an Iranian researcher who has published numerous dietary supplement studies. Many of them do not stand up to close scrutiny. Several have been retracted.
“That’s
almost 50 papers per year,” says Gaby. “Just on face value, that level of
productivity should raise a red flag.”
Further,
Asemi’s output indicates that he was simultaneously running as many as five
RCTs looking at five different treatments, concurrently. “That is unprecented.
In my decades of reviewing scientific papers, I’ve never come across anyone as
remotely prolific as this.”
Asemi’s
numerous citations cover nutrients and herbs including quercetin, ginger,
probiotics, magnesium, zinc, Vitamin D, berberine, and melatonin. He and his
colleagues claim they’ve used these to treat an equally wide range of disorders
including metabolic syndrome, diabetes, depression, leukemia, osteosarcoma, and
polycystic ovary syndrome (PCOS).
Papers
by Asemi and colleagues have found their way not only to obscure open-access
journals, but into some well-reputed high-impact ones like the American
Journal of Clinical Nutrition, the Canadian Journal of Diabetes, and
the British Journal of Nutrition.
Gaby
says the alarm bells about Asemi’s research are loud and numerous.
Beyond
the implausibly prolific output, nearly all of his 191 trials show
unequivocally positive, “statistically significant” outcomes for the
interventions being tested. Often the effect sizes are large—larger than one
usually sees in legit nutrient studies.
Further,
Asemi’s trials often have implausible time lines. “At least 12 of his papers
were submitted to journals before it was possible to have completed the trials.
That’s easy to determine because he says exactly when he started them, and how
long they lasted.”
For
example, a 2018 study of
magnesium and zinc for women with PCOS, published in the journal Biological Trace Elements Research,
states that recruitment was from June to August 2017, and that the treatment
period was 12 weeks. If recruitment ended on August 1 2017, the earliest that a
12-week trial could have been completed would be October 24 2017. Yet the journal
received the paper on Sept 27 2017—weeks before the treatment protocols could
be completed.
“I
looked up some data to see if that was even possible. The region where this
study was conducted (a city called Arak), has a population of about 500,000.
And I looked up the prevalence of gestational diabetes, and the birth rates for
this area. What I calculated was that during any given 3-week period, only
about 36 women in the entire city would have had gestational diabetes between
24 and 28 weeks’ gestation. Yet Asemi claimed to have recruited 60 such women
at just one clinic.”
Reluctance
to Retract
Gaby
shared his concerns about Asemi with the New Zealand team that ultimately took
down Sato and Iwamoto. The group obtained a grant to undertake an exhaustive
review of 172 studies by Asemi and colleagues. The result? A comprehensive
115-page dossier which the Auckland group sent to editors at 65 journals. It
details the myriad inaccuracies, implausibilities, discrepancies, and ethical
breaches spanning Asemi’s career.
Progress
has been slow, but as of now 12 of Asemi’s papers have been retracted, and
editors have issued 85 Expressions of Concern.
Gaby
says there are dozens of other Iranian researchers whose work is just as
questionable. There’s Reza Safarinejad, an internationally known urologist,
whose main interest is male infertility. He’s published numerous studies on the
impact of coenzyme Q10 (ubiquinol) on semen parameters, sperm function, and
pregnancy rates. He’s also published on omega-3s, selenium, and N-acetyl
cysteine for male fertility. According to Gaby, nearly all of Safarinejad’s
studies are problematic.
He points
to one in particular: a 2009 paper in
the Journal of Urology looking at the effect of CoQ10 on sperm parameters and hormone
levels in 212 infertile men.
Safarinejad
is the only author of this paper, and claims to be the sole treating physician.
Gaby holds that 212 is an implausibly large cohort for a stand-alone urology
practice doing its own non-funded research (no funding source is listed). “A
single investigator does not have the time or resources to conduct such a large
trial by himself.”
The protocol
was equally implausible: It claims that all 212 men visited the clinic 12 times
over a period of 13 months, and gave two semen samples at baseline, and two
samples within a 1-2 week period around each visit. Further, the semen was
collected after 3 days of recommended abstinence.
Implausible
Protocols
“That’s
24 semen samples per subject, with a total of at least 72 days of abstinence
over a 13-month period. I don’t know anybody who would do that. If somebody is
infertile and wants to have a pregnancy, he’s going to want to have intercourse
and have a baby. The idea that anyone would sign up for this (protocol) is
crazy,” says Gaby.
There
are also big logistical questions, like the process for collecting the samples.
“While half the 24 semen samples could potentially have been collected during
the 12 clinic visits, the other half (12 samples) would have to be collected
between visits. That is, at home. The subjects would have to deliver the
samples to the clinic within 1 hour of ejaculation, because sperm cells start
to die off after an hour. So, they would have to get to the clinic within one
hour, on 12 different occasions. The paper claims 194 of the 212 men completed
the trial and provided all the required 24 samples. That defies belief.”
Safarinejad
claimed that he and a lab tech did all the semen analyses. Doing the math,
that’s 4,650 sets of lab tests, all of which had to be done within hours of
ejaculation. That’s a heavy workload even for someone not running a busy
clinic.
Further,
the study’s inclusion criteria states that men were eligible to participate
only if they had “normal” fertile female partners “according to investigation.”
That meant the women had undergone a complete medical history, physical exam,
lab testing, and hysterosalpingogram.
“Doing
this on 212 women would be very expensive and time-consuming. It is not
something a urologist would do, so it would be done by a gynecologist. But the
paper does not specify who conducted these fertility evaluations and who paid
for them. And since Safarinejad is the sole author, and there’s no indication
of funding source, it defies the imagination that 212 women would have had salpingograms
just so their husbands could participate in a study.”
Dr.
Gaby sent a letter to the editors of the Journal of Urology detailing
his concerns. “They wrote back by email within 3 hours saying they were going
to investigate this. It took about 6 months, but a couple months ago they
issued an Expression of Concern about all 14 papers that Safarinejad had
published in their journal.” It’s slow progress, but this is several steps in
the right direction.
The
examples cited above are but a few. Gaby says he’s identified many more
problematic studies from Iran and from other countries. And keep in mind that
the US is definitely not immune to bad research.
Corrosion
of Trust
Fraudulent
research corrodes public trust in science; it misleads clinicians; and it skews
metanalyses and systematic reviews. Once marketers and sales people get hold of
it, they easily turn dodgy data into dishonest and misleading product claims.
At minimum, that means ordinary people get ripped off. At the extreme, people
could get hurt.
There’s
no lack of dubious research on pharmaceuticals, but the problem is especially
damaging to the field of natural medicine which is continually fighting for
credibility in the eyes of the broader medical community, the public, and the
regulators. Fraudulent studies like those described in this article bolster the
critics who want to paint the entire supplement industry as dishonest and
maleficent.
As is
easily seen from Dr. Gaby’s experience, and the New Zealand group’s efforts,
medical journals are reluctant to retract studies once they’re published. People
don’t like to admit they’re wrong, and retractions make journals—and their
editors—look bad. Plus, there could be potential accusations of libel, even
lawsuits.
Even
if papers are retracted, their negative impact lingers, especially if they’d
been in the literature for a long time, they appeared in high-impact journals,
and they were included in metanalyses.
Despite
his extensive experience exposing fraudulent research, Dr. Gaby stresses that
most nutrition/supplement researchers are honest, and most studies are clean.
“Most
nutrition research is believable, and the incidents of fraud do not change my
observation that nutritional medicine is highly beneficial for prevention and
treatment of a wide range of health conditions. But this is a stain on
scientific integrity.”
GLP-1
receptor agonists like Ozempic and Wegovy have rapidly become some of the most
widely prescribed drugs for weight loss and metabolic disorders.
While
they can sometimes be valuable aids in helping people normalize their weight
and their glucose metabolism, the mechanism of action for these drugs can have
some unhealthy consequences.
Many
people are now looking for alternative ways of boosting endogenous GLP-1
release.
In
this free webinar, we’ll discuss the four main issues with Ozmepic and other
GLP-1 drugs, and we’ll propose several natural alternatives, including: Berberine,
R-lipoic acid and BrocElite® sulforaphane.
We’ll
cover:
The four main health down-sides associated with Ozempic
The potential role of Berberine in weight management
The benefits R-lipoic acid and weight loss
The microbiome-modulating benefits of BrocElite® broccoli sulforaphae.
Eczema (Atopic Dermatitis) in a 34-year-old woman before, and after 3 months following a comprehensive naturopathic treatment program including dietary and lifestyle changes, and a range of botanical medicines and supplements aimed at reducing inflammation, restoring gut health, and improving gut and skin barrier function. (Images: Julie Greenberg, ND, Center for Integrative & Naturopathic Dermatology, Los Angeles)
Eczema
is seldom life-threatening, but it can have profoundly detrimental impact on
the people it affects. Clinicians who can bring a holistic, root-cause approach
to this common condition can make a big difference in the lives of their
patients.
“Roughly
20 million Americans have eczema. It’s a huge population. Patients are
desperate for help, and very few practitioners are providing holistic,
functional dermatology care,” says Julie Greenberg, ND, founder of the Center for Integrative & Naturopathic
Dermatology,
Los Angeles.
Severe
eczema, aka atopic dermatitis, causes significant physical suffering, disrupts
sleep, and often leads to social isolation and depression. Some patients find
it difficult, if not impossible, to work. That means the disorder can cause
long-term economic hardship.
Julie Greenberg, ND, RH (AHG)
“It’s
not just a little rash. It can really impact lives,” said Greenberg in a webinar hosted by Integrative
Practitioner. “These patients are motivated, they’re compliant, they really
want to get better,” Dr. Greenberg said. One of her severe eczema patients once
told her, “If you tell me to eat dirt, I’ll eat dirt.”
Dr. Greenberg, who is also a registered herbalist with the American Herbalists Guild (AHG), has years of experience treating severe skin disease exclusively with diet, lifestyle change, and botanical medicine. Through her Root Cause Dermatology training program she’s teaching other clinicians to do the same. The need for this, she says, is tremendous.
Boiling
Over
The
word eczema derives from the Greek “Ekzein”, meaning to “boil over.” The
very name implies heat, inflammation. And that, says Greenberg, should be the
central focus of treatment.
She stressed
that chronic skin problems like eczema are rarely just skin problems. In
nearly all cases, there are underlying systemic problems that warrant
attention. “It is a disease of skin barrier dysfunction, but also a disease of
deep systemic inflammation.”
Think of eczema as “leaky skin,” which is directly analogous and often concurrent with leaky gut.
While
it is important to quell the obvious symptoms and give patients some measure of
relief, it is equally important to identify and mitigate the drivers of
inflammation. As with all chronic inflammatory diseases, the specific drivers
vary from patient to patient.
Not
Just Th2
To
effectively treat eczema, you need to start with the pathophysiology says Dr.
Greenberg.
The
standard immunological view is that eczema is a Th2-mediated disorder. Th2
immune responses are typically triggered by helminths, fungi, and allergens,
and mediated by cytokines like IL4, IL5, and IL13.
It
is generally true that people with eczema do show Th2 predominance, and many of
the drug therapies for eczema, including the injectable biologics, squelch the
Th2 response. “Compared with psoriasis, it (eczema) is completely different.
Psoriasis does not have a Th2 component.”
But
Dr. Greenberg stressed that eczema is not always exclusively a Th2 disease. “It
can have a Th1 or Th17 component as well.”
Th1
responses are typically driven by intracellular bacteria, viruses, and
protozoa, while Th17 responses are usually driven by extracellular bacteria and
fungi at mucocutaneous sites. Some people even show a Th22 pattern, suggestive
of tissue inflammation.
In
evaluating people with eczema, it’s important to take all these factors into
consideration.
Immunological
Endotypes
Greenberg
cited a 2019 review by Tali Czarnowicki and colleagues that looked at
immunological endotypes in diverse populations with atopic dermatitis.
They
compared European-American, Asian-American, and African-American cohorts, and
found that while all showed Th2 features, the Asian-Americans were more likely
to show Th17 responses than European- or African-Americans.
There
were also age-related differences: pediatric patients were more likely than
adults to show Th17 responses. These are just a couple of the endotype patterns
that Czarnowicki discovered. The point is, atopic dermatitis may not be as
uniform as we previously thought. This suggests that treatments also need to be
individualized and tailored to immunological endotype, rather than simply to
lesion severity (Czarnowicki
T, et al. J Allerg Clin Immunol. 2019)
Atopic dermatitis (AD) endotypes. This composite image shows clinical phenotypes, polar cytokine activation cartoons, immune polarization of T-cell subsets, and epidermal barrier changes for each AD phenotype. Intrinsic (Int), extrinsic (Ext), acute (A), and chronic (C) subtypes were characterized only in European-American patients with AD, and thus appear exclusively under this category. Epidermal barrier measures, including epidermal thickness, keratin 16 (KRT16), Ki67, FLG, LOR, and periplakin (PPL), were similar in patients with intrinsic and extrinsic AD, but more evident in European-American patients with chronic versus acute AD. (From, Czarnowicki T, et al. J Allerg Clin Immunol. 2019)
“An
attempt to define the patient’s endotype before treatment should be made to
optimize therapeutic responses moving toward precision medicine based on the
different clinical and molecular disease subsets,” writes Czarnowicki. “Although
Th2 axis activation seems to be a universal trait across the AD spectrum, it
still might be the case that other or additional cytokine targeting will be
highly effective for a particular subset of patients who present a distinct
endotype.”
The
Role of Food Allergies
Dr.
Greenberg called food allergies the “elephant in the room” in eczema. Though it
is not accurate to say food allergies ‘cause’ the disease, they certainly can play
a role in driving the process and triggering flares.
“It’s important to consider, but strictly focusing on food triggers is less likely to give you strong traction in adults with eczema. Food eliminations can help some people, but it’s not a cure-all.
But
again, the impact of food allergies—which can be IgG-, IgA-, or IgE-mediated–varies
widely between patients. Age is a factor in this: allergies play a much more
prominent role in infants and young children than they do in adults with eczema.
According
to Thomas Werfel and Kristine Breuer at the Hannover Medical University,
Germany, well over 50% of children with atopic dermatitis experience
exacerbations in association with particular foods (Werfel T, Breuer K. Curr Opin Allergy Clin Immunol. 2004).
But adolescents
and adults are far less likely to experience food-associated flares. Dr.
Greenberg estimated that two-thirds of all adult eczema patients do not
show signs of allergy to food or environmental allergens. That’s partly because
people tend to outgrow childhood allergies to milk, eggs, wheat, soy, and other
common allergens. Further, by the time people reach their 20s and 30s, they’re usually
aware of their problem foods, and they tend to avoid them.
“It’s
important to consider, but strictly focusing on food triggers is less likely to
give you strong traction in adults with eczema. Food eliminations can help some
people, but it’s not a cure-all. Try it and see. But if food elimination is not
working, not giving total clearance, don’t get stuck. You need to dig deeper.”
Dairy
is No Friend
What’s
the most common culprit food group? Dairy.
“When
patients do experience food-related eczema flares, 75% are due to milk or
dairy,” Dr. Greenberg said, adding that when taking a patient’s history, it is
really important to ask about all forms of dairy, not just milk.
“If
you ask about “milk,” patients will think you mean drinking glasses of milk.
They’ll say “no.” But then later you’ll find out that they eat a lot of cheese.
So, ask about anything that’s produced by a mammal mamma for a baby, and that
includes sheep and goats too.”
Without restoring gut health, it is difficult if not impossible to maintain skin health.
Greenberg
says she encourages all her eczema patients to eliminate dairy. They might not
all be frankly allergic to it, but as a food category dairy is seldom doing
them any good. “I’ve yet to meet an eczema patient for whom dairy is doing any
favors. So, I just take it out.” Other common trigger foods are wheat/gluten,
eggs, peanuts, and soy.
“Wheat
is 50/50. Some patients are sensitive, some are not. Stool testing and organic
acid testing will usually show it,” she said. Regarding eggs, the degree to
which people experience flares is often “dose dependent.” Most can eat eggs
occasionally without flaring, but eating them several times per week or more increases
the risk of flares.
For
some patients, wine and especially red wine, can be problematic. “It’s high in
histamines, and high in yeast. In patients with fungal overgrowth, you don’t want
to give more yeast,” Dr. Greenberg said. Further, alcohol converts to sugar
which fuels inflammation.
Does
Eczema Cause Allergies?
We
could also ask whether eczema causes food allergies, says Dr. Greenberg. “It’s
a weird way to think about things, but we think that this is likely.”
Food
sensitization problems are 6 times more common in kids who have eczema compared
with those who do not, according to a study by Tamara Strugar and colleagues (Strugar TL, et
al. J Drugs Dermatol. 2019). Generally speaking, the eczema develops first, then the food
allergies and sensitivities.
Any type
of skin barrier disruption during infancy positively predicts the emergence of
food allergies by age 2. Dr. Greenberg noted that kids who have eczema early in
life are also much more likely to develop asthma than those without eczema.
Based
on a systematic review of 66 separate studies, Teresa Tsakok and colleagues at
the St. John’s Institute of Dermatology, London, estimate that one-third of all
children with early onset eczema go on to develop food allergies, asthma, or
both, later in life (Tsakok
T, et al. J All Clin Immunol. 2016). Researchers have described this
as the “Atopic Triad.”
Leaky
Skin, Leaky Gut
What
are the connections? Think of eczema as “leaky skin,” which is directly
analogous and often concurrent with leaky gut.
The
skin is constantly in contact with the external world, exposed to a host of
potentially noxious substances such as environmental toxins, pollen, food
allergens, viruses, mites, animal dander, plant irritants, and the like. “They’re
outside us. They shouldn’t get in. They shouldn’t reach the dendritic cells. And
when the skin is healthy, they don’t get in and the immune system remains calm,”
she explained.
Eczematous
skin is characterized by breaches in the epidermal barrier. Things that should
be on the outside get down into deeper layers where they reach the dendritic
cells, and this generates the various types of T-cell responses.
The
same thing is happening in the gut. Dr. Greenberg noted that each time we
swallow—a phenomenon that happens roughly 2,000 times per day—we are bringing
the “outside” world inside the body.
A
healthy, well-functioning digestive tract has multiple mechanisms—stomach acid,
mucus production, microbiome factors, tight junctions between endothelial
cells—for preventing noxious stimuli from entering into the bloodstream and the
tissues.
“In
a leaky gut, there’s a breach of the mucosal layer and the lumenal contents get
in, which is very inflammatory, leading to further breakdown of the mucosal
barrier. Things get into the bloodstream that do not belong there.
Lipopolysaccharides get through
and activate
the dendritic cells, causing the release of IL6, TNF alpha, IL1-beta, which drives
inflammation.”
Treat
the Gut
Whether
the initial barrier breakdown is in the skin or in the gut, the key to
long-term resolution of eczema lies in careful assessment and treatment of the
latter. Without restoring gut health, it is difficult if not impossible to
maintain skin health.
“I test
and treat the gut in all my eczema patients,” says Dr. Greenberg. “I run a
stool (microbiome) test and an organic acid test on every single patient I see,
right before the first visit. As a naturopath, I’m interested in their digestive
function, so I look at markers for what’s going in, and what’s coming out. I
look at how someone’s extracting and absorbing nutrients from what he or she is
eating.”
She
says she pays close attention to several key aspects of gut health, including:
Oral and Nasopharyngeal
Microbiome: Though the intestinal microbiome dominates research and popular
discussions about probiotics, it is only one part of the overall picture. Many
problems begin upstream, with the oral and nasopharyngeal microbiomes. Dr.
Greenberg advises checking the oropharynx. Is there evidence of gingivitis?
Chronic nasal or sinus infection? Has the patient had extensive dental work?
Root canal therapies? All of these
factors may play contributing roles in the underlying inflammation.
Stomach acid
production: Many people with eczema are hypochlorhydric. They’re not
producing enough stomach acid, which means that potentially problematic
microbes that would normally be destroyed in a properly acidic stomach, are
getting through to the intestines. The problem is amplified in those who carry Helicobacter
pylori, and those on acid-blocking drugs.
Evidence of
dysbiosis:
Eczema patients often show overgrowth of certain commensal organisms, an absence
of beneficial bacteria, and/or the presence of pathogenic bugs.
Microbiome
Factors
A
healthy human intestinal tract will show robust populations of Faecalibacterium
prauznitsii—an important producer of butyrate—and Akkermansia
mucinophila—which eats old mucus and stimulates endothelial goblet cells to
produce more mucus.
Eczema
patients almost always show low levels of both. That means they’re usually
deficient in butyrate, which is produced by F. prauznitsii as it
ferments dietary fiber. Butyrate is the preferred fuel of enterocytes, and it
also quells inflammation. The absence of A. mucinophilia means the gut
is less able to repair and restore its protective mucus layer.
Many
eczema patients also show relatively low levels of beneficial organisms such as
Bifidobacteria and Bacteroidetes, but overgrowth of Staphylococcus
aureus, various species of Streptococcus, Escherichia coli,
and fungi like Candida albicans.
These
microbiome changes are evident very early in life. Lotte Nylund and colleagues
at the University of Turku, Finland, showed that infants with severe atopic
dermatitis have far lower levels of butyrate-producing bacteria in their GI
tracts than do healthy infants and those with mild AD (Nylund L, et al. Allergy.
2015).
Generally
speaking, the severity of atopic disease is inversely correlated with GI
microbial diversity, and with the presence of butyrate-producing organisms.
A
Role for Probiotics
Given
these relationships, it’s reasonable to think that probiotic supplementation
could be helpful in treating eczema. Dr. Greenberg says they do have a role,
but on their own, they are seldom going to result in complete resolution of
skin symptoms, especially in severe eczema.
“I use
probiotics, but it’s definitely not the only the only thing,” she said.
Clinical
studies are conflicting. The most comprehensive paper on this topic–a 2019
systematic review of 44 separate trials of probiotics in atopic patients–came
to a split conclusion: 50% of the studies showed benefits from probiotics, but
the other 50% showed no effect (Petersen E, et
al. Acta Dermatol Venereol. 2019).
That
stalemate is due in part to the extreme heterogeneity of the studies included
in the review: probiotic strains, doses, and treatment durations varied widely
from trial to trial.
Dr.
Greenberg said some of her own patients have been getting good results from a
relatively new probiotic product
containing live Akkermansia mucinophilia. Made by Pendulum Health, this is the
only product on the market providing the live form of this important organism.
But
again, Akkermansia probiotics are not a cure-all. Greenberg said she often uses
spore-based probiotics as well. And she insists that her patients get at least
35 grams of dietary fiber per day, either from food, supplements, or a
combination of the two. “I make all my patients take a lot of fiber. Most
people really lack it in their diets.”
Tackling
Candida
Candida
is a big culprit in people with eczema.
GI
overgrowth of candida shows a statistically significant correlation with IgE
antibodies in atopic dermatitis patients (Savolainen J,
et al. Clin & Experimental Allergy. 1993). The authors
of this study noted that “Severe phases of AD in colonized patients are
associated with IgE synthesis against C. albicans.”
When
AD patients who do have IgE antibodies to Candida are treated with
antifungals, the skin symptoms improve. This was shown 25 years ago, in a study
by a team of dermatologists at Hiroshima University School of Medicine in Japan
(Morita E, et
al. J Dermatol. 1999).
“I
find this 100 percent,” said Dr. Greenberg, referring to her own experience
treating Candida in people with eczema.
Keep
in mind that in addition to triggering a shift from Th1 to Th2 immunological
patterns, the presence of fungi like Candida at mucocutaneous sites will
also drive Th17 reactions. Many people with leaky gut will show Th17 reactions,
and these are associated with autoimmune conditions. It’s important to keep
this in mind.
Candida overgrowth is
very common among people with eczema. “Get the Candida down, and the
skin gets a lot better,” says Dr. Greenberg. She stressed that she treats
fungal infections via dietary changes and herbal antifungals such as Rosemary (Salvia
Rosmarinus), Pau d’arco aka Lapacho (Handroanthus impetignosus), and
Uva Ursi (Arctostaphylos uva-ursi).
H. Pylori: A Hidden Culprit
Be
on the lookout for Helicobacter pylori in your eczema patients, says Dr.
Greenberg.
Electron micrograph of multiflagellate Helicobacter pylori. (Image: Yutaka Tatsumi, MD, Dept. of Pathology, Fujita Health University School of Medicine)
Roughly
half of all people carry H. pylori, and for many, it seems to cause no
harm. This has led some researchers to view it as a benign commensal. But for some people, this bug is highly
problematic. It’s association with peptic ulcers, gastritis, and gastric cancer
are well-known. Fewer people are aware that it is also linked to skin diseases
like rosacea, chronic urticaria, eczema, severe acne, and alopecia areata.
H.
pylori can
produce lipopolysaccharides and endotoxins, as well as biofilms, all of which
can be problematic, especially in people who already have compromised mucosal
barriers and systemic inflammation.
It also
produces urease and other substances which create a buffer against stomach
acid. This allows the organism to live in a very low-pH environment that
normally would be utterly hostile for bacteria. In other words, it diminishes
one of the body’s primary defenses against noxious stimuli from the outside
world. The neutralization of stomach acid also leads to suboptimal digestion,
which has downstream consequences.
“Stomach
acid signals to the pancreas and gall bladder to produce bile and enzymes. A
deficit of stomach acid leads to suboptimal production of enough bile, pancreatic
enzymes,” Dr. Greenberg explained. “That’s not good for us.”
Diagram depicting H. pylori embedded in the mucus layer of the stomach, and producing urease. The enzyme catalyzes a reaction between urea and water, resulting in ammonium and bicarbonate, which neutralizes stomach acid, thus promoting the survival and growth of the organism. (Image by Olivia Child/Wikimedia Commons)
This
acid-mitigating effect ensures H. pylori’s own survival, and it also
enables potentially problematic protozoans like Giardia and Entamoeba
to survive the stomach and enter the intestines.
Protozoans
are common findings in stool analyses of people with eczema, and these patients
almost always have H. pylori.
Are
the protozoans always pathogenic? No, but Dr. Greenberg says she errs on the
side of treating them as such. Her go-to botanicals for eliminating protozoans
are Artemisia and Black Walnut (Juglans nigra). Likewise, she
considers H. pylori to be an etiologic factor in eczema, and treats it
accordingly, even if the patients do not have peptic ulcers or gastritis. Her
preferred herbs for mitigating H. pylori are: Mastic gum,
deglycyrrhizinated licorice (DGL), and black cumin (Nigella sativa).
The
Ear Infection Connection
There
is a strong connection between chronic ear infections and eczema. Dr. Greenberg
noted that most children with eczema also have frequent ear infections. And if
you ask, you’ll find that many adults with eczema have histories of chronic ear
infections in childhood.
The
reasons for the association might not be obvious. But embryologically, it makes
sense. The bones of the middle ear, and the eustachian tubes develop from the
first and third pharyngeal arches which are the developmental foundation of the
head and neck, including the pharynx. The eustachian tubes themselves open into
the nasopharynx.
This
means there’s a fundamental anatomical connection between the ears, the
digestive, and the respiratory tracts. We think of them as separate systems,
but actually, they are interconnected.
In a
recent review paper, Amy S. Graham and colleagues at the Neuroscience
Institute, University of Cape Town, South Africa, explored these connections in
detail, coining the term “Auditory-Gut-Brain Axis.” They suggest that changes
in the gut microbiome, chronic inflammation, and disorders of the ear and of
auditory processing, may all be related (Graham AS, et
al. Front Neurosci. 2023).
On
the patient care level, Dr. Greenberg reported that she’s had a number of
eczema patients who experienced complete clearing or at least significant
improvement of ear infections after eliminating dairy and wheat as part of a
lifestyle program to mitigate the eczema. “I started to advise my ear infection
patients to cut out wheat and dairy, even if they don’t have eczema. Many have
gotten better.”
Assessing
Eczema Patients
In
addition to a thorough history and physical exam, Dr. Greenberg’s initial
assessment depends on two cornerstone tests: the GI-MAP
(Microbial Assay Plus), a PCR-based test to detect the presence of various bacteria,
fungi, viruses, worms, and protozoa in fecal samples; and an Organic Acid
Test, to
assess overall nutrition status, metabolic function, detoxification capacity,
and neurotransmitter status.
“Every
patient has to do the GI-MAP and the OAT before the first visit. I use these as
a baseline. It’s immensely helpful. Depending on the clinical history, and
initial evaluation, I might order other tests as well.”
Other
potentially useful tests include the DUTCH tests
(Dried Urine Test for Comprehensive Hormones); Mold and mycotoxin tests; Hydrogen or methane
breath testing for small intestinal bacterial overgrowth (SIBO); Food allergen
tests; and specific tests to assess intestinal permeability.
“I
use the labs as a roadmap. I know where we’re starting: severe eczema. And I
know where we want to go: clear skin. The findings from the labs give clues on
where to focus treatment-wise.”
Individualizing Treatment
Given
the range of immunological endotypes, microbiome factors, and potential food
and environmental triggers that can contribute to the pathogenesis of eczema,
an effective treatment program must necessarily be individualized, says Dr.
Greenberg. She adds that resolution of chronic eczema takes time, and that she
typically shifts the focus of treatment every 2-3 months.
“These patients are motivated, they’re compliant, they really want to get better”
The
fundamental goals of treatment are to quell systemic inflammation, eliminate
inflammatory triggers, eliminate pathogens, restore a healthy gut,
oropharyngeal, and skin microbiomes, and repair damaged skin and gut mucosa.
She
stressed that as a naturopathic physician, she does not use prescription drugs,
but is able to achieve excellent results with lifestyle modification, dietary
changes, food trigger eliminations, herbal antimicrobials, and probiotics.
“You
have to go deep. It’s far beyond prescribing tubes of steroids or Th2 response
inhibitor drugs. That’s all just system suppression. You push down the Th2
response, you push down the inflammation. But you’re not really finding and
treating the root causes. You can’t just treat from the outside in, you have to
also work from the outside in.”
She
added that the general approach she takes with eczema patients will often work
well for those who have psoriasis and other chronic skin disorders.
Irritable Bowel Syndrome (IBS) and Osteoporosis are two of
the most common conditions that integrative practitioners see among their
patients. These disorders are actually related.
The common factor? Bone Morphogenic Proteins (BMPs)—a group
of cytokines that play important roles in bone and joint homeostasis as well as
in GI mucosal integrity.
In this free webinar, Cynthia Worden, DO, will explore the connections
between IBS and Osteoporosis, and share new insights into the dual role of Bone
Morphogenic Proteins in supporting patients with GI and bone health issues.
She’ll also describe her clinical experience with Ostinol®–the
only BMP-complex available for oral supplementation.
During this webinar, you’ll learn about:
The epidemiological
relationship between IBS and Osteoporosis—and the rising rates of both
conditions
The discovery of BMPs, their
structure, and their function within Demineralized Bone Matrix
Mechanisms of action and
observed clinical impact of BMPs
The practical benefits of
BMPs in supporting patients with IBS and Osteoporosis
Case studies & clinical
experience with Cyplexinol®
Musculoskeletal Regenerative Nutrition
SPONSORED BY Regenerative Tissue Sciences, the professional sales division of ZyCal Bioceuticals Healthcare Co., Inc.
Cynthia
Worden, DO, MSHPE, IFMCPearned her medical degree at Western
University of Health Sciences in Pomona, CA in 2004. She also completed a
teaching fellowship in Osteopathic Manipulation, a Master’s in Health
Professions Education, and a Doctorate in Osteopathy. Dr. Worden completed her Internship and
Osteopathic Family Medicine residency training at Downey Regional Medical
Center.
Following her training, she practiced
Integrative Family Medicine at Creekside Family Practice in Portland, OR, for
10 years. After discovering functional
medicine, Dr. Worden realized it held many of the answers to her patient’s
chronic medical conditions. She became a Certified Practitioner with the
Institute for Functional Medicine (IFMCP) in 2016, after which she founded
Bloom Functional Medicine in 2018.
Like many
who practice functional medicine, Dr. Worden has faced her own health issues:
Hashimoto’s and Crohn’s disease. Consequently, she has first-hand
knowledge of how these conditions affect overall health and well-being. In her
free time, she loves to spend time with her family and friends, and to continue
her learning. She loves to cook, read, kayak, ski, hike, and travel.
Obelisk S.s: A novel viroid-like entity discovered within Streptococcus sanguinis, a facultative anaerobe that is part of the normal oral flora. According to the Stanford University researchers who discovered them, Obelisks represent an entirely new phylogenic category (Image from: Zheludev IN, et al. BioRxiv.com. 2024)
Just
when you thought the microbiome couldn’t get any weirder, investigators at
Stanford University have discovered a whole new dimension in the microbial
universe: a category of distinct, self-replicating RNA sequences in and among bacteria
of the human gut and oral microbiomes.
Named
“Obelisks” owing to their circular rod-like structures, these peculiar bits of
genetic information are unlike any genomic sequences in the known viral,
bacterial, fungal, or animal worlds.
In
discovering Obelisks, Nobel prize-winning geneticist Andrew Fire and his team believe they’ve opened an entirely new frontier in
microbiology.
“Obelisks form
their own distinct phylogenetic group with no detectable sequence or structural
similarity to known biological agents,” they write in their newly published article on
bioRxiv.com, the Cold
Spring Harbor Laboratory’s preprint server platform.
A New
Frontier
So
far, Fire and his colleagues have identified almost 30,000 distinct Obelisks, by
applying a bioinformatics tool called VNom (Viroid Nominator) to databases containing 5.4 million genome sequence datasets.
Obelisks
are diverse in structure, but they share several common features. They’re all
circular RNA strands of no more than 1kb in length. That’s tiny even by the
miniscule standards of molecular biology. They form predictable rod-like
secondary structures. And they contain open reading frames that code for unique,
previously unknown protein-like entities that the Stanford group has named
“Oblins.”
In analyzing
microbiome data sets representing the oral and gut microbiomes of 472 healthy human
donors, they found that nearly 10% of these individuals carried one or more
Obelisks among their commensal bacteria. These curious RNA sequences were more
prevalent in oral versus gut microbiome samples (53% versus 6.6%), which suggests
that the oral flora may be a reservoir for Obelisks in humans.
Streptococcus
sanguinis, a
facultative anaerobe that is part of the normal oral flora, is the first
bacterium within the human microbiome that the Stanford team has identified as
a definite host for Obelisks. The specific Obelisk subtype that Fire and
colleagues discovered inside S. sanguinis, is able to replicate, and to
produce a certain type of Oblin within the Streptococcal cells.
“Obelisks form their own distinct phylogenetic group with no detectable sequence or structural similarity to known biological agents.”
–Andrew Fire, Professor of Molecular and Genetic Medicine, Stanford University
This,
they say, is clear evidence that Obelisks can and do live—if such entities can
be considered living–within bacterial cells. Though other bacterial hosts for
Obelisks have not yet been identified, Fire says “it is reasonable to assume
that at least a fraction (of the Obelisks) may be present in bacteria.”
Obelisks
are Everywhere
Inside or outside of bacterial
host cells, Obelisks seem to be everywhere. The Stanford group has
detected them, at varying prevalence levels, in metatranscriptomes from people living
in the US, Canada, Brasil, China, India, Russia, and Australia, as well as
several countries in Europe and Africa. They’ve also found them in non-human
mammals, fish, birds, arthropods, even in soil and sediment. Wherever there is
life of any sort, there appear to be Obelisks.
Geographic distribution of viroid Obelisks as indicated by counts of non de-replicated SRA (Sequence Read Archive) datasets arranged by sample geolocation (where known) illustrated on a world map (darker orange = more SRA datasets). SRA counts are not expected to correlate with true geo-/ecological prevalence, but are still indicative of global presence. ( Zheludev IN, et al. BioRxiv.com. 2024)
Are Obelisks friendly? Fearsome?
Both? At this point, nobody knows.
They
do share some structural traits with viroids—the small, non-encapsulated DNA or RNA strands typically found in
plants, and which are sometimes pathogenic. The potato spindle tuber viroid
(PSTVd), and the citrus exocortis viroid (CEVd) are two common examples of
pathogenic plant viroids.
Like
viroids, Obelisks are very small circular RNA sequences that lack protein coats.
This absence of a protective protein capsule is the key feature that
distinguishes both viroids and Obelisks from true viruses.
So
far, none of the 29,959 Obelisks discovered by Fire and his team appear to
cause harm to the bacteria among which they’re found, or to their human
meta-hosts. And there’s not yet enough information about them to determine
whether they are helpful.
Are Obelisks friendly? Fearsome? Both? At this point, nobody knows.
It
is clear that Obelisk RNA sequences can be transcribed into protein-like structures,
but the function of these so-called Oblins is an open question.
The Stanford
researchers have found only one such Oblin that has an identifiable function: a
self-cleaving ribozyme similar to the hammerhead
type-III ribozymes. Hammerhead ribozymes are RNA catalytic cleavage sequences found in
genomes throughout the bacterial, viral, and eukaryotic realms.
Beyond that,
almost everything else about Obelisks and Oblins is a mystery at this point.
A Cornucopia
of Questions
Lead
investigator Andrew Fire is no stranger to the frontiers of knowledge. In 2006,
he and his colleague Craig Mello won a Nobel Prize in Physiology or Medicine
for their discovery of RNA interference (RNAi)—a mechanism
that regulates gene expression. At the time, their elucidation of RNAi
revolutionized scientific understanding of how genomes self-regulate. Their
work underscored the ways in which tiny bits of double-stranded RNA can turn
off gene transcription.
Nobel Prize winning genticist, Andrew Fire, Professor of Molecular & Genetic Medicine, Stanford University
In
the years since, Fire and his group have continued to delve into the mysteries
of RNA, and they’ve developed sophisticated methods for detecting previously
unidentified RNA sequences. It is this work which led to the discovery of
Obelisks.
In his
new paper, which has yet to be peer-reviewed, Fire acknowledges that the discovery
of RNA Obelisks raises a cornucopia of interesting questions: How do Obelisks
replicate? How do they move from extra- to intracellular environments? How many
different Obelisk subtypes are there and what do they code for? What types of
bacteria are most or least amenable to hosting Obelisks? Do the Oblins
transcribed from the Obelisks have any important biological functions?
In microbiome data sets representing the oral and gut microbiomes of 472 healthy human donors, nearly 10% of these individuals carried one or more Obelisks among their commensal bacteria.
There
are also big questions about how Obelisks affect the microflora in and around
which they dwell, and by extension, the higher organisms that host these
commensal microbes.
“Are Obelisks plasmid-like in that they
can co-exist, and in some cases, contribute to host adaptability and fitness?”
Fire asks. “Are they largely a deleterious or beneficial element to harbour?
And what impact, if any, does harbouring an Obelisk have on ‘meta’-host
physiology? Is Obelisk positivity predictive of human health states?”
Again, the answer to all of these
questions is: We don’t yet know.
A New ‘ome?
It is notable that Obelisk prevalence,
like microbiome composition, varies by anatomic site: the presence of Obelisks
is much higher in the oral versus the intestinal microbiome.
Obelisks may—at least in part—be
“colonists” within specific types of bacteria, in a similar way that various commensal
bacteria have specific preferences for colonizing particular organ systems.
By way of rough analogy, the Obelisks might
be something akin to the microbiome’s microbiome.
Dr. Fire speculates that if that proves
to be the situation, then “donor-specific factors such as diet or lifestyles therefore likely play a role in
Obelisk (re-)colonisation and retention.”
Predicted Obelisk secondary structures depicted as “jupiter” plots where chords represent predicted basepairs (coloured by basepair probability from 0, grey, to 1, red, see methods) with predicted open reading frames (ORFs, preceded by predicted Shine-Delgarno sequences, purple) depicted. ( Zheludev IN, et al. BioRxiv.com. 2024)
He adds that further study of S.
sanguinis will be an important line of research in clarifying the
relationship between these newly discovered RNA agents, the various microbiomes,
and human physiology.
“Study of the implied S. sanguinis-Obelisk relationship might begin to reveal the relevance of Obelisks to the natural oral niche and potentially to human health, as well as offer a tractable model system to study Obelisk molecular biology.”
On the Threshold of Life
Researchers now know vastly
more about the interrelationship between commensal microbes and human
physiology than they did 20 years ago. But the Stanford group’s discovery of
viroid Obelisks underscores just how much there is yet to discover about the
invisible worlds that shape our existence.
This is especially true of
viruses and related entities. In fact, the virome may be even more complex, influential, and downright
weird than the bacterial microbiome.
According to an article by
UC San Diego’s David Pride, and Rockefeller University’s Chandrabali Ghose, there are an estimated 380 trillion
viruses inside the average human body. That’s ten times the
already staggering number of bacteria in the typical human microbiome.
The overwhelming majority of viruses and
viroid particles appear to be harmless. Those that are harmful are usually
pathogenic to specific species. There are very few examples of viruses that
cause disease throughout the animal kingdom.
Some viruses may actually be helpful.
Researchers now know that genes from viruses known as HERVs (human endogenous
retroviruses) account for up to 9% of the total human genome.
Obelisks appear to dwell at the threshold
between entropy and order, between the realm of living things and the vast
universe of inanimate matter. Their discovery is a brilliant burst of light
into a domain that researchers have termed “viral dark matter.”
So far, early responses to the discovery
from microbiologists and molecular biologists have been enthusiastic and
positive. Beatriz Navarro, a plant viroid expert based at the Institute for
Sustainable Plant Protection in Bari, Italy, praised it as “impressive,” in an interview published in New Scientist.
“Really
wild and cool discovery for virus nerds,” gushed Steven Salzberg, a
biostatistician at Johns Hopkins University.
Computational biologist Simon Roux, at the DOE Joint Genome Institute at Lawrence
Berkeley National Laboratory, told the
journal Science that he is “really impressed
by the approach” that Fire and colleagues took in their work.
Roux is among a group of
scientists who surmised that viroids—or similar non-encapsulated entities—might
exist beyond the botanical world, inside commensal bacteria. The Stanford
discoveries give credence to that hypothesis.
He added that the discovery of
Obelisks begs the important question of whether true viruses evolved out of
things like Obelisks and viroids, or rather the other way around–that Obelisks
and viroids are the result of de-evolution of viruses or other more complex
forms of life.
It
will probably be years before we know if Obelisks have a role in human health
or illness. But it is clear that their discovery is the first step in what will
likely be a long and exciting scientific odyssey.
Fresh, versatile, and nutrient-packed, Broccoli also turns out to be good medicine. A new analysis of NHANES data from more than 5,500 Americans indicates that eating broccoli once or twice per week can reduce all-cause mortality by 32% to 43%. (Image: voyager_human/Shutterstock)
Imagine if there were a drug that could reduce risk of cancer and cardiovascular disease by roughly 40%, without any adverse effects. Even better, people would only need to take it 2 or 3 times per week to obtain these preventive benefits.
It turns out there is such a thing. It’s called broccoli.
People
who regularly eat broccoli once or twice weekly can reduce their all-cause
mortality by an impressive 32% to 43%, according to a new analysis of data from
more than 5,500 US adults.
Frequent
broccoli consumption had a particularly strong impact on deaths from cancer and
cardiovascular disease, according to a collaborative research team based at the
Jilin University Hospital, Changchun, and the Beijing Shijitan Hospital,
Capital Medical University, Beijing.
“Consuming
broccoli 1–2 times per week for males and 3 or more times per week for females
could significantly reduce all-cause mortality risk,” report
Xiangliang Liu and co-authors. They suggest that, to a
point, broccoli consumption may confer something like a “dose-response” effect
on death rates from common diseases: the more frequently someone eats this healthful
crucifer, the greater the mortality reduction.
They
base that conclusion on a detailed study of data from 12,486 Americans in the
NHANES (National Health and Nutrition Examination Survey) 2003-2006 cohort. The
NHANES project uses an extensive Food Frequency Questionnaire (FFQ) to gather
detailed dietary information from participants. The FFQ includes two questions
specifically about broccoli: “Have you ever consumed broccoli?” and “How
frequently do you consume broccoli?”
A
total of 5,556 participants in the 2003-2006 NHANES cohort (2,743 males and 2,813
females) provided complete responses to these broccoli questions. All were over
20 years of age; 30% were over age 65.
Based
on those responses, Dr. Liu and colleagues divided the cohort into four
categories: never
consumers (N=739), infrequent consumers who ate broccoli “less than once a
week” (N=3,181), occasional consumers, defined as “1 to 2 times per week but
less than 3 times per week” (N=1,216), and regular consumers, meaning those who
ate broccoli “3 or more times per week” (N=420).
Impact
on CVD & Cancer
During
the 10-year follow-up period, which ended December 31, 2019, there were a total
of 1,405 deaths from all causes among the 5,556 subjects (25.3%). Cardiovascular
disease caused 504 deaths (35.9%), and cancer accounted for 292 deaths (20.7%).
There were 107 deaths (7.6%) attributed to pulmonary/respiratory diseases, with
the remainder attributed to accidents, renal disorders, diabetes, or
“miscellaneous causes.”
After
applying three different statistical models to control for a wide range of other
variables associated with increased mortality, such as age, gender, race,
education level, socioeconomic status, body mass index (BMI), smoking, and
alcohol consumption, Liu and colleagues saw a clear signal: broccoli intake is
inversely correlated with mortality.
In
the statistical model with the strictest controls on potentially confounding
variables, they found that compared with people who said they never ate
broccoli, those who ate it occasionally (less than once weekly but several
times per month) had an all-cause mortality hazard ratio of 0.7—a 30% risk
reduction. For those who ate broccoli 1-2 times per week, the hazard ratio dropped
to 0.58. That’s a 42% risk reduction.
But
among the broccoli-lovers, who reported eating it 3 or more times per week, the
hazard ratio was 0.72 compared with never-eaters, a finding that suggests the
risk-reductive effect plateaus at a certain intake frequency, beyond which
there’s no further gain.
Looking
specifically at cardiovascular risk, they found a similar pattern: compared
with never-eaters, those who ate broccoli occasionally had a 21% risk
reduction, and those who ate it 1-2 times weekly had a 38% risk reduction.
The
cancer data also showed this pattern: those who ate broccoli occasionally had a
30% lower risk of cancer-related mortality than the never-eaters. For those who
ate it 1-2 times per week, the hazard ratio was reduced by 41%. Among the most
frequent broccoli eaters, the risk was also reduced by 41% compared with
non-eaters, again suggesting that the protective effect reaches a plateau (Liu X, et al. Front
Nutr. 2008).
Gender
Differences
Dr.
Liu and his colleagues saw a distinct gender-based difference in the pattern of
risk-reduction: Males seem to obtain a greater benefit at lower consumption
frequency than females. The latter need to eat broccoli at least 3 times per
week to gain the all-cause mortality reduction that men get from once or twice
weekly intake.
The
reasons for this difference are not entirely clear, but the authors do offer a
couple of speculations about it:
“On
the one hand, the intake of fruits and vegetables is inherently higher in
females’ diets, so they may need to eat broccoli more frequently to produce
significant health effects. On the other hand, increased estrogen levels can
promote the expression of glutathione peroxidase, enhancing the body’s
antioxidant capacity, which may make females require higher amounts of
antioxidant nutrients in broccoli.”
Putting
it simply, women tend to have higher antioxidant intake along with higher
inherent antioxidant capacity than men do. Therefore, to see an impact on
mortality, women would need to eat substantially more broccoli than men.
A field of Broccoli (Image: Andrii Yalanskyi/Shutterstock)
A
True Superfood
The
risk reductions reported by Liu and colleagues are impressive in their
magnitude, but they should not be entirely surprising: broccoli is an extremely
fiber-rich and nutrient-dense vegetable. The authors cite a number of key nutrients
within broccoli which likely play a role in its risk-mitigating effects:
High levels of direct antioxidants such as
vitamin C, carotenoids, and anthocyanins, that can quench oxygen-free radicals
and mitigate oxidative stress.
Sulfur-containing phytochemicals like
glucosinolate, which inhibit the production and release of inflammatory
mediators, and which also stimulate production of antioxidant enzymes.
Sulforaphane, which promotes insulin signal
transduction in the liver and in skeletal muscle, thus improving insulin
sensitivity and regulating blood glucose.
High levels of vitamin K1, a fat-soluble
vitamin that promotes production of clotting factors while inhibiting the
synthesis and secretion of cholesterol from the liver.
A wealth of flavonoids that can scavenge free
radicals and accelerate cholesterol breakdown.
High levels of water-soluble mucilaginous fiber,
that can prolong gastrointestinal transit time and improve digestion, bind bile
acids, and slow the absorption of carbohydrates, thereby preventing
post-prandial glucose and insulin surges.
Rich in minerals, especially magnesium, which
can reduce cholesterol absorption.
“Adequate
intake of broccoli helps maintain the functionality of pancreatic beta cells,
preventing insufficient insulin secretion due to pancreatic cell injury and
thus stabilizing blood glucose regulation,” the authors stated. “By regulating
glucose and lipid metabolism and enhancing insulin sensitivity, broccoli can
reduce the risks of metabolic syndrome, type 2 diabetes, and cardiovascular
diseases.”
To some degree, Dr. Liu’s team was able to quantify the anti-inflammatory effects of broccoli consumption. Using blood samples obtained from the NHANES participants, they measured monocyte, lymphocyte, platelet, and neutrophil counts, and found a clear reduction in the neutrophil-to-lymphocyte ratio—a key cellular marker of inflammation—associated with increased broccoli intake.
“Substantial
evidence indicates that chronic inflammation and oxidative stress play
important roles in the pathogenesis of various chronic diseases, including
cancers, cardiovascular diseases, and type 2 diabetes,” Liu and colleagues
state in their report. “Therefore, the abundant anti-inflammatory and
antioxidant components in broccoli may be important nutritional mechanisms for
its beneficial effects against chronic diseases.”
Who’s
Eating Broccoli?
In
their analysis, the Beijing researchers found several interesting demographic
disparities in frequency of broccoli consumption within the NHANES cohort:
women tended to eat it much more frequently than men, and non-Hispanic whites
ate it more often than other racial/ethnic groups.
There
was also a surprising relationship between socioeconomic status (as indicated
by poverty income ratio) and broccoli consumption: those in the middle range
tended to eat more broccoli than those at the low and the high ends of the
socioeconomic spectrum.
Like
any epidemiological study based on diet questionnaires and self-reporting, this
one too has methodological limitations. The authors acknowledge the possibility
of recall bias and participant subjectivity, which should be taken into
consideration when drawing conclusions about the data.
Even
with those limitations in mind, it is clear that regular broccoli consumption
has a significant impact on reducing death rates from cardiometabolic and
neoplastic disease. Pharmaceutical executives dream of finding novel drugs that
can knock 30% or 40% off the mortality rates from common diseases.
Quantifying
“Food as Medicine”
By
studying the relationship between consumption frequency and disease-associated
mortality rates, Liu and colleagues are, in a sense, attempting to quantify the
concept of “food as medicine.”
They
note that while there have been many studies of broccoli and other cruciferous
vegetables over the decades, and most show positive health impacts. But few
prospective studies have looked specifically at the effects of low, moderate,
and high intake levels.
In
the introduction to the study, they point out that “the available data do not
provide specific recommendations for broccoli consumption frequency. Therefore,
it is of great significance to use large sample prospective study results to
analyze the dose–response relationship between broccoli intake frequency and
all-cause and cause-specific mortality, which can provide guidance for dietary
adjustment in different populations, especially dietary interventions for
patients with chronic diseases.”
Though further research is needed, not just on broccoli, but on other ‘healthy’ vegetables, Liu’s study makes a strong case that men who eat broccoli once or twice weekly, and women who eat it three or more times per week, are doing themselves a great favor.
“Die Nurnberger Gesetze”: A chart published in 1935, outlining racial categories defined by the Nazis’ Nuremberg Race Laws. Under these laws, only full-blooded “Aryan” Germans (“Deutschbluetiger”) were considered citizens. Jews (“Jude”) in Germany lost their citizenship and were ultimately exiled or rounded up for execution. “Mixed race” (“Mischling”) people of various “grades” were similarly disenfranchised and persecuted. “Racial hygiene” laws were at the core of public health under the Nazis. (Image: US Holocaust Memorial Museum).
How did the most sophisticated and scientifically advanced medical system of its time become an agency of systematic state-sanctioned mass murder?
Issued
in early November, to coincide with the 85th anniversary of Kristallnacht—the
violent pogroms generally considered to be the start of the Nazi effort to
exterminate the Jews —The Lancet’s report is the most thorough
exploration of this troubling subject to date.
Richard Horton, MD, Editor in Chief, The Lancet
Richard
Horton, MD,The Lancet‘s Editor-in-Chief, convened the
20-member
Commission on Medicine, Nazism, and the Holocaust to develop “a reliable,
up-to-date compendium of medicine’s and medical professionals’ roles in the
development and implementation of the Nazi regime’s antisemitic, racist, and
eugenic agenda, which culminated in a series of atrocities and, ultimately, the
Holocaust.”
Co-chaired by
medical historians Herwig Czech, of the
Medical University of Vienna, and Shmuel
P. Ries, MD,
of the Hebrew University Hadassah Medical School, Jerusalem, the commission
included physicians, historians, and medical ethicists from Austria, Spain,
Germany, Israel, Czech Republic, Poland, and the United States.
“Medical
crimes committed in the Nazi era are the best-documented historical example of
medical involvement in transgressions against vulnerable individuals and
groups. What happened under the Nazi regime has far-ranging implications for
the health professions today, and virtually every debate about health
professional ethics can gain from an understanding of this shameful history,” the
authors write in their introduction.
The
Lancet report emerges at a time when many
people glibly throw around terms like “Nazi” and
“genocide,” and
“concentration camps” in
political discourse to support a range of often
opposing causes and positions.
Deliberately inflammatory use of such words is clearly displayed on both sides
of the discourse about the current Israel-Hamas conflict.
Just 3 years ago, the same sort of button-pushing language arose
during the Covid pandemic, when some opponents of vaccine mandates invoked the
specter of Nazi medical experiments to make their case. It has come up
repeatedly in debates about healthcare reform, where opponents of national
healthcare decry “government death panels.”
Medical historian Herwig Czech, Medical University of Vienna
The Lancet’s report
also comes at a time of widespread Holocaust denial, when the ranks of those
who actually experienced the horrors of World War II are growing thin, and the global
geopolitical order is increasingly unstable.
In light of all of this, it behooves us
all to learn what actually happened in Germany and surrounding countries from
1931 to 1945.
Exclusion From Healthcare
The
atrocities of the Holocaust were the culmination of longstanding cultural and political
movements in which “science, medicine, and public health were used to justify and
implement persecutory policies and eventually state-sanctioned mass murder and
genocide.”
The Lancet committee defines the latter term as “the targeted
murder of specific religious, racially defined, national, or ethnic groups.”
The
report traces the origins of these movements from their roots in late 19th
Century European “race science,” through their dissemination during the tumultuous
Weimar-era of German history, and ultimately through their operationalization as
national policy after 1933, when Hitler took power as Germany’s chancellor.
The
Weimar period was a time of great political and economic strife in Germany, and
in much of Europe. It was also a time of rapid scientific and technological
advances, as well as social change. During that period, the ranks of German
medicine included a growing number of Jews, women, and non-German immigrants.
The Lancet report cites a 1933 German census showing that while Jews
comprised roughly 1% of the nation’s population, they represented roughly 10%
of its doctors. Not everyone was happy about that.
One
of the new Reich’s first formally racist anti-Jewish policies was a general
boycott of Jewish-owned businesses–a call that explicitly mentioned Jewish
physicians’ practices.
This
was quickly followed by the 1933 Law for the Restoration of the Professional Civil Service, which forbade
Jews from holding positions in the civil service, including the public health
service, and at universities, which included medical schools. The Lancet
committee states that this led to the immediate dismissal of nearly 20% of all
people working in academia, 80% because they were Jews and 20% because they
were deemed enemies of the Nazi regime.
Further legislation in April and June of 1933, explicitly excluded Jews and other “political opponents” from receiving payments from the nation’s health insurance system. By 1938, the Reich stripped all Jewish physicians of their medical licenses, made it illegal for them to call themselves doctors, and forbade them from treating non-Jewish, ethnically German patients.
From
Genetics to Genocide
Though
extermination of Jews was always part of Hitler’s plan, the industrial scale
mass murder that we’ve come to know as the Holocaust did not begin with Jews,
or for that matter, with the Roma, Sinti, homosexuals, or political prisoners
all of whom ultimately became victims of the Nazis’ agenda. Rather it emerged
out of the Reich’s eugenics program, and it began with forced sterilization of
people with physical disabilities and psychological disorders.
Cover of the September 1937 edition of Neues Volk (“New People”) idealizing pure-blood Aryan motherhood. Neues Volk was a Nazi publication promoting eugenics, racial hygeine and other aspects of Nazi ideology. (Image: US Holocaust Memorial Museum)
At
the core of the Nazi ideology was the concept of the Volk—a idealized,
heroic, racially superior German people that had been unjustly dethroned and
debased by an “international order” imposed by the Allied powers after World
War I, and which must re-assert its dominance first in the German homeland,
then in Europe and beyond.
This
doctrine was framed in a context of racial hierarchy, defined according to a
set of physical, mental, and temperamental traits. The so-called Aryan and
Nordic races at the top, and the African races, as well as the Slavs, the Roma,
and the Jews, were at the bottom. Hitler and the Nazis held a particular
contempt for Jews, blaming them for Germany’s defeat in WWI and labeling them
as a nefarious racial “enemy within” bent on weakening and destroying the Volk.
Central
to Nazi policy was the notion of “racial hygiene” (Rassenhygiene),
a medico-social ideology rooted in genetics and social Darwinism, which
viewed human affairs as an existential competition between races, and which obligated
the German Volk to promote procreation of its most “fit” people, while
simultaneously purifying itself from those deemed “racially undesirable” or
“genetically unfit.”
This
was formerly codified in the Nuremberg Laws of 1935, which
stated that only people of “German
or related blood” were eligible to be Reich citizens, and which forbade
intermarriage and interracial sexual intercourse. It also imposed a wealth tax
of up to 90% on Jews or any other newly disenfranchised people who sought to
emigrate out of Germany.
Nazi poster depicting a stereotyped Jewish male as a threat to the racial purity of an Aryan woman. The term “Rassenschande” translates as “race defilement”.
Under these
laws, couples had to obtain certificates of “biological fitness” before they could
marry. Access to all public social support services was closed to all
individuals deemed impure or unworthy.
Responsibility
for enforcing the Law for the Protection of German Blood and German Honour –one
of the two key Nuremberg Laws–fell largely on the public health offices. The
practice of medicine in this context became an endeavor to strengthen the Volkskörper
(the German national body) and prepare it for the arduous task of conquest and
empire-building.
A
1939 public health service handbook stated that “Every measure, undertaken in
all areas, must be examined from the point of view of population policy, and
care for heredity and race.”
In
essence, the Nazi racial hygienists—many of whom were physicians–sought to
apply principles gleaned from the nascent science of genetics, and from
centuries of animal husbandry, to control human reproduction. The Lancet
report notes that Rudolf Hess, Hitler’s deputy Führer, once described National Socialist doctrine as,
“applied
biology,” and called the regime a “biopolitical dictatorship.”
Christine Neemann, an Aryan German woman, and Julius Wolff, a German Jewish man, being publicly humiliated in Norden, Germany, 1935. The couple was engaged to be married, in violation of the Nuremberg Laws. Nazi police officers forced Wolff to wear a sign stating “I am a race defiler.” Both Neemann and Wolff were sent to concentration camps, which they somehow survived. (Image: US Holocaust Memorial Museum).
“Applied
Biology” & “Ballast Lives”
Eugenics
was the practical manifestation of racial hygiene. By 1931, even before Hitler
took power, the writings of three German racial theorists—Erwin Baur, Eugen
Fischer, and Fritz Lenz—were compiled into a multi-volume textbook, the title
of which translates as: Human Heredity Theory and Racial Hygiene
This
book was a cornerstone of Nazi public health policy. It codified the notion
that left unchecked, “lower races” could—and would—contaminate “higher races”
leading to physical and social degeneration. To prevent this, the racial
hygienists called for the outlawing of racial mixing, and the elimination of
“counter-selective forces.” That meant people of mixed-race heritage, people
with hereditary illnesses, those with physical or mental disabilities, and
those with irremediable character flaws like alcoholism and drug addiction.
These
people were considered “ballast lives” (Ballastexistenzen)”—people with
no inherent worth, who weighed down the healthy body politic.
The
Reich enacted the Law for the Prevention of Hereditarily Diseased Offspring
in 1933, which called for the forced sterilization of women and men who were physically
or mentally disabled, “criminally insane,” or “feebleminded.” That latter was a
catch-all term applicable to many different types of people the regime
considered unworthy.
Another cover of Neues Volk magazine, this one advocating euthanasia for people with disabilities. The text reads: “This hereditarily ill person will cost our national community 600,000 Reichmarks over the course of his lifetime. Citizen, this is your money.” (Image: US Holocaust Memorial Museum)
“Physicians
(especially psychiatrists) and other health professionals not only spearheaded
the crafting of the sterilisation law, but also played crucial roles at each
step of implementation. Their contribution to the law’s enforcement began with
the mandatory reporting of patients judged to be hereditarily diseased,” write
the Lancet commission authors. Medical practitioners also carried out
the sterilization procedures, typically done surgically or via x-ray exposure.
The
Lancet
points out that the principles of eugenics had wide currency at the time, not
just in Germany, but in many other parts of the world. In fact, the Nazis’
sterilization law was partly based on legislation drafted by American eugenicist Harry Laughlin. Indeed, 12 US
states including Indiana, Connecticut, Virginia, Oklahoma, and California, had
forced sterilization laws on the books at some point in the early 20th
Century.
The Nazis’ anti-Black
racial policy led to the extralegal forced sterilization of an estimated
600-800 children born to White European mothers and African fathers who had
served as soldiers during the French occupation of the Rhineland after WWI.
The
Lancet
authors estimate that in total, between 310,000 and 350,000 people were forcibly
castrated or ovarectomized under the Nazi eugenics program. But sterilization
was just the beginning.
In
1939, the Reich authorized Aktion T4, “a centrally organised patient
mass murder programme.” Named forTiergartenstraße 4, the Berlin address where the program was headquartered, this policy
mandated “mercy deaths” for people with disabilities, mental illnesses, or any
other sort of incurable condition.
Physicians
and midwives were mandated to provide the government with detailed information
about all children with disabilities, who would subsequently be assessed by medical
panels tasked with selecting which children could be “remediated” and which were
to be killed. Under the Reich Committee for the Scientific Registration of
Serious Hereditary and Congenital Diseases, the state established a network
of 30 “special children’s wards” where children were given “good deaths” to
free them from “lives not worth living.”
Map of Aktion T4 “euthanasia” centers in and around Germany from 1940-45. Run by doctors and other medical personnel, these centers were sites for the systematic mass murder of hundreds of thousands of people deemed “unworthy of life” owing to physical or mental disabilities or alleged genetic diseases. (Image: US Holocaust Memorial Museum)
Between
1939 and 1945, an estimated 300,000 adult patients in psychiatric hospitals
throughout Germany, Austria, occupied Poland, and other regions of Eastern
Europe were culled and exterminated under Aktion T4. The infrastructure
and methods for mass murder which defined the Holocaust —including the use of poison
gas—were developed under Aktion T4.
And
all of this was willingly overseen and implemented by medical personnel.
Willing
Physicians
The
Lancet
authors point out that no civilian physicians were forced to participate in the
T4 program, and that “many in the psychiatric elite advocated for the killing
of patients deemed incurable, to enable specialists to focus on patients who
could be healed and thus improve the reputation and influence of their
profession.” Others who participated willingly were motivated by an ardent
belief in Nazi ideology and racial hygiene theory.
One
such enthusiastic participant was Hans Asperger, the Viennese
pediatrician notable for his groundbreaking studies of atypical neurology in
children, and for whom the Asperger Syndrome is named.
Asperger
was a self-avowed “Austrofascist,” and Catholic eugenicist. During WWII he was
one of many doctors who evaluated children according to their fitness or
unfitness for integration into the German volk. Those he deemed unfit,
he sent to the Am Spiegelgrundclinic
(literally the “mirror-ground”), a T4 killing site in Vienna. During the war
years, 789 children at Am Spiegelgrund were “euthanized” via gas
poisoning, lethal injection, or deliberate starvation.
Image from a Nazi state propaganda film promoting the Reich’s Aktion T4 “euthanasia” program. The text reads: “…because God cannot want the sick and ailing to reproduce” (Image: United States Holocaust Memorial Museum)
In
addition to racial hygiene, there were also economic rationalizations for the
state-sanctioned killings. By eliminating the “incurable,” hospital beds and
medical resources would be made available for treating wounded soldiers, or
Germans with treatable conditions.
Many
victims of Aktion T4 were ethnic Germans, and by 1940, people within
Germany—including the influential Catholic leader Archbishop
Clemens August Graf von Galen –voiced opposition to the program. This prompted the regime to
officially end it in 1941, at least on paper. In reality, the systems set in
motion by Aktion T4 simply continued in the concentration camps that the
Nazis built for extermination of Jews, Roma, gay people, political prisoners,
and others.
Nazi racial hygienist Eva Justin assessing a Romani family imprisoned in a “Zigeunerlager” (“Gypsy Camp”) near Vienna in 1940. Along with the Jews, the Nazis deemed the Romani people to be racial enemies. Millions of Romani and Sinti were murdered, deported, and imprisoned. (Image: US Holocaust Memorial Museum)
The
Lancet
report notes that many medical personnel who ran T4 kill centers were
reassigned to concentration camps. One example is Irmfried Eberl, an Austrian
physician who ran two T4 “clinics,” and who was subsequently transferred in
1942 to the notorious Treblinka camp in Poland. In a period of 6 weeks, Eberl
oversaw the murder of approximately 280,000 Jews. He was dismissed for failing
to effectively conceal the realities of Treblinka from the neighboring
villages.
Human Experiments
Beyond
their role in justifying, systematizing, and facilitating mass murder, Nazi physicians
and biomedical researchers also established a heinous program of
experimentation on human subjects.
This,
the Lancet commission points out, is especially ironic because at the
turn of the 20th century, Germany was the first country to institute
formal medical ethics guidelines for human research.
Back
in 1900, the Prussian Ministry of Cultural Affairs issued a ruling against
experimentation on humans without consent, in response to a scandalous
experiment in which healthy women and children had been intentionally exposed
to syphilis. It came three decades before the notorious Tuskegee study in which
US Public Health Services researchers deliberately infected 400
African-American men with syphilis.
In
1931, the German Ministry of the Interior posted guidelines requiring that
human subjects give explicit consent to participate in research, and only after
appropriate instruction and education.
Though
these rules were technically still in force under the Nazis, the new Reich
interpreted them as applying only to members of the “German national body, but
not to those excluded from it.” Enemies of the volk deemed “untermenschen”
(literally, “under-men” or “subhuman”), were fair game for research.
Josef Mengele (center) was the most notorious perpetrator of medical atrocities during the Nazi period. As chief physician at the Auschwitz-Birkenau concentration camp complex, he routinely selected prisoners and new arrivals for extermination, and also conducted a series of medical experiments known for their extreme cruelty. He is flanked by Richard Baer (commandant of Auschwitz, May 1944 – Jan 1945), and Rudolf Höss (commandant of Auschwitz from May 1940 – Nov 1943). Image: US Holocaust Memorial Museum
The untermenschen—a
term the Nazis applied to Jews, Roma, Slavs, Blacks, mixed-race people,
homosexuals, people with disabilities, Communists, anti-Nazi dissidents, and
prisoners of war–were human enough for any data obtained from them to be
relevant to the German volk, but not human enough to be protected under guidelines
limiting human experimentation.
Medical
historian Paul Weindling and colleagues have carefully documented 300 human experiments
involving at least 27,000 people, conducted by Nazi physicians and researchers
during the war. These experiments covered a broad range of scientific questions.
But they all aligned with core Nazi doctrines and goals: supporting the war
effort, achieving German economic autarchy, eastward expansion of the Reich, and
strengthening the health of the German race.
Research
on concentration camp inmates included studies of physiology under extreme
physiological stress like hypothermia or high altitude; control of infectious
and insect-borne diseases; effects of chemical and biological weapons; human
reproduction and mass sterilization; genetics and hereditary biology.
Josef Mengele is the most
notorious Nazi physician. He oversaw the prisoner “selections” at
Auschwitz-Birkenau, determining who was fit for forced labor and who was to be
gassed immediately. He headed the “infirmary” in the camps, where he ran a
number of experiments on prisoners.
Mengele
was particularly interested in identical twin sets, using one twin as the
experimental subject and the other as the control. Among his goals was to aid
racially-superior couples to produce more twins thereby speeding the growth of
the Aryan population.
He
was also determined to develop blood tests that could reliably and irrefutably detect
someone’s race. And he also ran disinfection and disease control studies which
involved deliberately infecting prisoners in order to test experimental
treatments.
“Mengele’s
research practices were marked by extreme brutality and a complete disregard
for the humanity of the people forced to participate, as well as the
unscrupulous exploitation of the resources and atrocious context of the
Auschwitz camp,” write the Lancet authors. The doctor was known as Todesangel
(Angel of Death) for good reason.
“New
Opportunities, Deregulated Spaces”
Mengele
may have been extreme in his ruthlessness, but he was certainly not unique in
his zeal.
“Medical
scientists interested in pursuing research projects were generally aware of
what they saw as new opportunities for research in the deregulated spaces
created by the Nazi regime, where legal and ethical rules could be ignored,”
writes the Lancet commission.
Gynecologist Carl Clauberg (left) who oversaw fertility experiments on women imprisoned in Auschwitz (Image: US Holocaust Memorial Museum)
One
example is Carl Clauberg, a gynecologist and fertility researcher who specifically
requested permission from SS director, Heinrich Himmler, to set up a
sterilization research project in Auschwitz. Similarly, SS physician Karl
Gebhardt saw his assignment to Ravensbrück as an opportunity to test new
sulfonamide drugs on prisoners of war deliberately inflicted with
“standardized” wounds intended to simulate battle wounds.
The
concentration camps were also a boon for anatomy labs at German universities.
According to the Lancet report, academic centers now had easy access to
human cadavers from the euthanasia programs, forced labor camps, and
concentration camps.
A
Catalog of Horrors
The 70-plus
page Lancet report is a catalog of horrors difficult to fathom. Yet each
statement in the report is referenced and well-substantiated. In aggregate, the
evidence clearly shows “the cooperation between civil medical research
institutions, military medicine within the German armed forces and SS, and the
pharmaceutical industry.”
The
report dispels several widely held, comforting notions that propagated widely
throughout the medical world in the post-war era. One is that the medical
atrocities carried out by the Nazis were the work of a small number of radical
fanatics—the “a few bad apples” thesis.
Though
there were many medical professionals who did resist the racist policies of the
Reich, the Lancet report shows that the majority of physicians willingly
participated.
“The historical
evidence provided here will show that physicians joined the Nazi Party and its
affiliated organisations in higher proportions than any other profession,” the
authors note, adding that, “The convergence of professional interests with
political motives partly explains the gravitation of many physicians towards
Nazism: by 1945, 50–65% of German physicians had joined the Nazi Party, a much
higher proportion than in any other academic profession.”
Waldemar Hoven, chief SS doctor at the Buchenwald concentration camp, testifying during the “Doctors Trial” in Nuremberg, June 23, 1947. Hoven ran Aktion T4 programs, as well as a series of typhus experiements on prisoners in the camp. He was found guilty of crimes against humanity and executed by hanging. (Image: US Holocaust Memorial Museum)
The Lancet authors also challenge the notion that the Nazis had no concept of medical ethics. In truth, all the horrors of the Holocaust occurred under a clearly articulated set of ethics crafted for the service of political, economic, and racial aims.
“Nazi Germany
developed a specific form of ethics that put the health of the German people
above all else, but that excluded vast numbers of individuals from being
considered part of the German people according to eugenic, antisemitic, and
other racist criteria. Thus, medical ethics became another instrument to help
design, rationalise, and implement the regime’s eugenic and racist agenda.”
Within its own racist
notions of public health, the Nazi medical establishment went to great lengths
to promote the wellbeing of the Volk. The Reich established one of the
world’s first public tobacco cessation campaigns, and it also actively promoted
healthy whole-food diets. It ran prenatal health services and family support
programs—but again, only for Germans deemed fit and worthy of them.
After the war,
23 Nazi medical personnel were brought to justice during the Nuremberg Doctors’ Trial of 1946-47,
and 7 were sentenced to death. But the vast majority of those who perpetrated
medical atrocities during the Nazi era—including Josef Mengele—were never
captured or prosecuted.
The sentencing of Herta Oberheuser, a doctor at the Ravensbruck concentration camp, during the Nuremberg Doctors Trial. Oberheuser, a dermatologist, ran ghastly infection experiments on prisoners. She was sentenced to 20 years in Landsberg Prison, but was released in 1952 for good behavior. (Image: US Holocaust Memorial Museum)
The Lancet
Commission on Medicine, Nazism, and the Holocaust: Historical Evidence, Implications
for Today, Teaching for Tomorrow is not an easy read. But it is an important one.
The
authors effectively describe how the horrors of Nazi medicine emerged not from
irrational rage, but from principles, ideologies, and worldviews prevalent
throughout academia in 19th century Europe.
As much as it
is a history lesson, the Lancet report is a cautionary tale.
The dangers of
overly reductionistic thinking, medical industrialization, and co-optation of
medical ethics by political agendas are with us today.
“In
the Nazi era, science, medicine, and public health were used to justify and
implement persecutory policies and eventually state-sanctioned mass murder and
genocide. Studying the history of medicine during Nazism reveals the dangerous
potentials of modern medicine, which coexist with medicine’s immense power to
benefit humanity. The significance of this history is not limited to the
descendants of the victims and perpetrators and their societies: it is relevant
to communities worldwide—not least because early 20th-century Germany pioneered
so many aspects of modern medicine that were adopted to varying degrees in many
countries.”